A man with chronic recurrent headaches using codeine

Headache
Pain
This case highlights some clinical issues arising from the rescheduling of codeine. A pain physician, an addiction medicine specialist and a neurologist discuss their own particular aspect of care of this patient who has chronic recurrent headache and has been self-medicating with over-the-counter codeine.
- A clear diagnosis of the cause of disabling headache is a vital first step. The most likely cause in this patient is migraine.
- A wide range of highly effective treatment options for migraine prevention and acute treatment are now available.
- Medication overuse headache is a superimposed complication of an underlying headache disorder, and opioids will need to be discontinued in this patient.
- Management requires patient education, supportive care and symptomatic or substitution medication.
- The rescheduling of codeine will present challenges in primary care but equally will contribute to the reduction of harm that opioids have on the community.
Case scenario
With codeine no longer being available over the counter, Jason is concerned that he will have to resort to pethidine injections like his mother needed for her ‘blinding headaches’. Jason finds his work as a chef quite stressful. He also has hypotension, which is made worse when he is in a hot environment. Jason asks whether medicinal cannabis might be a better alternative for his headaches.
Commentary from a pain medicine physician
By Diarmuid McCoy
Chronic headache is considered to be a chronic pain and the approach follows a similar pattern. The definition of pain is ‘An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage’.1 This has recently been considered for revision.2 The explanatory note is significantly longer than the definition indicating the complexity of the entity that is being managed. The definition does, however, highlight the importance of the psychosociobiomedical approach to the management of pain including headache.
Jason presents with a number of converging issues all requiring attention. These are:
- chronic headache
- dysfunctional medication use
- unsafe medication use
- occupation-related stress
- stress and anxiety around the change in regulations
- questions about the use of cannabis.
The diagnosis is of vital importance. Associate Professor Stark has outlined below a diagnostic approach for this case. Even with the confounding factor of medication overuse headache (MOH), the most likely cause is migraine.
The principles of the approach required are logical and straightforward. This approach is to diagnose, introduce more appropriate medication, monitor and discontinue opioids. The skills in communication and allowing adequate time to execute this approach will be crucial. Jason is still in the workforce, which should be seen as a positive factor. However, his job is stressful and the nature of his work is unlikely to change.
During the initial consultation, recording baseline questionnaires will be very useful in reflecting on progress later in his treatment. The Electronic Persistent Pain Outcome Collaboration (ePPOC) is a recognised minimum data set that has been used for this purpose (available online at https://ahsri.uow.edu.au/eppoc/forms/index.html). It can be scored easily and repeated to demonstrate change. It consists of four main questionnaires: the Brief Pain Inventory, which records pain intensity and interference; the Depression Anxiety Stress Scale; Pain Catastrophising Score and the Pain Self-Efficacy Questionnaire.
Introducing the concept of the multi-disciplinary approach will be of vital importance. The concept of seeing a psychologist may be resisted in the first instance. A psychologist may, however, be able to identify some triggers or exacerbating factors and in collaboration with the patient help develop strategies for identifying and managing them. Mindfulness cognitive behavioural therapy has been investigated for the management of headache including migraine and has demonstrated benefit.3,4
Jason may be fearful that a label of addict will be applied to him, therefore, the differences and overlap of the following definitions should be explained to him.
- Addiction:
—inability to consistently abstain
—impairment in behavioural control
—craving or increased ‘hunger’ for drugs or rewarding experiences
—diminished recognition of significant problems with one’s behaviours and interpersonal relationships, and
—a dysfunctional emotional response. - Tolerance: drug tolerance is a pharmacological concept describing a person’s reduced relief from an analgesic following its repeated use requiring an increase in its dosage to achieve the same effect.
- Dependence: a state in which a person only functions normally in the presence of the substance an experiences physical disturbance (withdrawal) when is it removed.
A discussion about addiction, tolerance and dependence presents an opportunity to establish a good therapeutic alliance with the patient and for the patient to appreciate that they are being taken seriously and feel validated and to give them the confidence to remain engaged with the process.
It appears clear even from the limited information in the case scenario that the codeine-containing medication is ineffective in managing Jason’s headache. This can be discontinued in the manner that has been outlined by Professor Lintzeris below. Pain-related education will include clarifying with the patient that not only is the codeine not helping but it is contributing to the headache and complicating it. In addition, the amount of paracetamol consumed on his ‘bad’ days is also a source of concern. Patients often underestimate the true amount and in a manner that is not deliberately deceptive. Withdrawal can often be achieved safely as an outpatient but may require frequent consultations. Admission to hospital may be required if the withdrawal symptoms become troublesome. Clonidine is useful in small divided doses in easing withdrawal symptoms, as is buprenorphine either sublingual or by patch.
The Faculty of Pain Medicine has produced a smart phone application to determine equivalent doses of opioid medications (http://fpm.anzca.edu.au/documents/opioid_calculator_app.pdf). The traffic light system on this app is useful in graphically illustrating the amount of opioid Jason is taking (16 x 15 = 240 mg codeine = 30 mg morphine + 8 g paracetamol). The paracetamol is a significant problem also and needs to be highlighted with the patient. The maximum advised dose per day is 4 g. Liver function tests should be carried out as a baseline at this stage and monitored in the future.
There is a family history of troublesome headache, which adds to the suspicion of the primary headache being migraine. In addition, his mother’s use of pethidine by injection needs to be explored further. This might indicate a risk factor for Jason in developing an opioid-related substance misuse disorder, not only related to the management of his headache but also in an attempt to decrease the stress of his work. Included in the history was the description ‘blinding headache’, which may be how Jason remembers his mother describing her migraines, but perhaps also reflects catastrophic reaction to pain (headache). This would be recorded in the Pain Catastrophising Score in the ePPOC questionnaire. Repeating the questionnaire will help document progress especially from the psychological perspective and serve as positive feedback.
Subcutaneous lignocaine in doses of up to 2500 mg over 24 hours is also beneficial in some patients. The use of triptans and other drugs has been discussed by Associate Professor Stark below. Intravenous lignocaine at a dose of up to 5 mg/kg over two to three hours has demonstrated some effect in patients with headache including migraine (note, lignocaine is used off label for migraine).5 Ketamine, an N-methyl D aspartate antagonist which is useful in some pain states, has not proven to be as effective in headache (off-label use). There does not appear to be a mechanical aspect to Jason’s headache and therefore blockade of the zygapophyseal joints in the cervical spine for cervicogenic headache is not indicated.
In the specialist care setting other measures including invasive therapies might be considered. These include spinal cord stimulation (high cervical spine), occipital nerve stimulation and transcranial magnetic stimulation.6 The number of patients suitable for these techniques is small. In recent years, in addition to injections of botulinum toxin type A (discussed below), percutaneous electrical nerve stimulation has demonstrated some promise. It is approved for use in Australia and the National Institute for Health and Clinical Excellence in the UK has supported its use. It consists of placing short solid needles (50 mm) in the subcutaneous tissues over the occipital nerves and sometimes over the supraorbital nerves. Treatment is generally repeated at intervals and can be undertaken as a hospital outpatient.
The final issue of the role of cannabis in this case is a common question. Although it is widely suggested that cannabis (medical/medicinal marijuana) is effective for a wide variety of pain conditions, the high-quality medical scientific evidence is unpersuasive. Begin this conversation by clarifying what the patient understands by medical cannabis. Currently there is no registered medical supplier of the product and the legislation for its use has yet to be finalised. On current evidence it is unlikely to be of benefit and may be associated with significant side effects.
Summary
Jason requires medical education about his current headache state.7,8 A reduction of his opioids and appropriate preventive and therapeutic measures are also needed. He may also need psychological intervention to manage anxiety and develop strategies for managing headache. He will need regular review.
Commentary from an addiction medicine specialist
By Nicholas Lintzeris
Jason’s case highlights three contemporary clinical issues arising from the rescheduling of codeine products and the increasing -community expectations of the availability of medicinal cannabis. These issues are the:
- identification and management of MOH
- assessment and management of possible opioid dependence related to use of over-the-counter codeine
- potential role and current approaches to using medicinal cannabis in Australia.
Medication overuse headaches
MOH is a severe form of chronic headache affecting 1 to 2% of the general population. It arises from overuse of acute headache medications, including opioids, triptans and even simple analgesics (e.g. paracetamol, NSAIDs). MOH is classified as headaches occurring on 15 days or more per month for more than three months, and where the headaches have developed or markedly worsened due to overuse of medi-cation (≥10 days/month of opioids).9 MOH usually occurs in the context of a poorly treated underlying headache condition (e.g. migraines, tension headaches), which after excessive long-term use of acute headache medications changes from an episodic -condition to chronic regular headache.
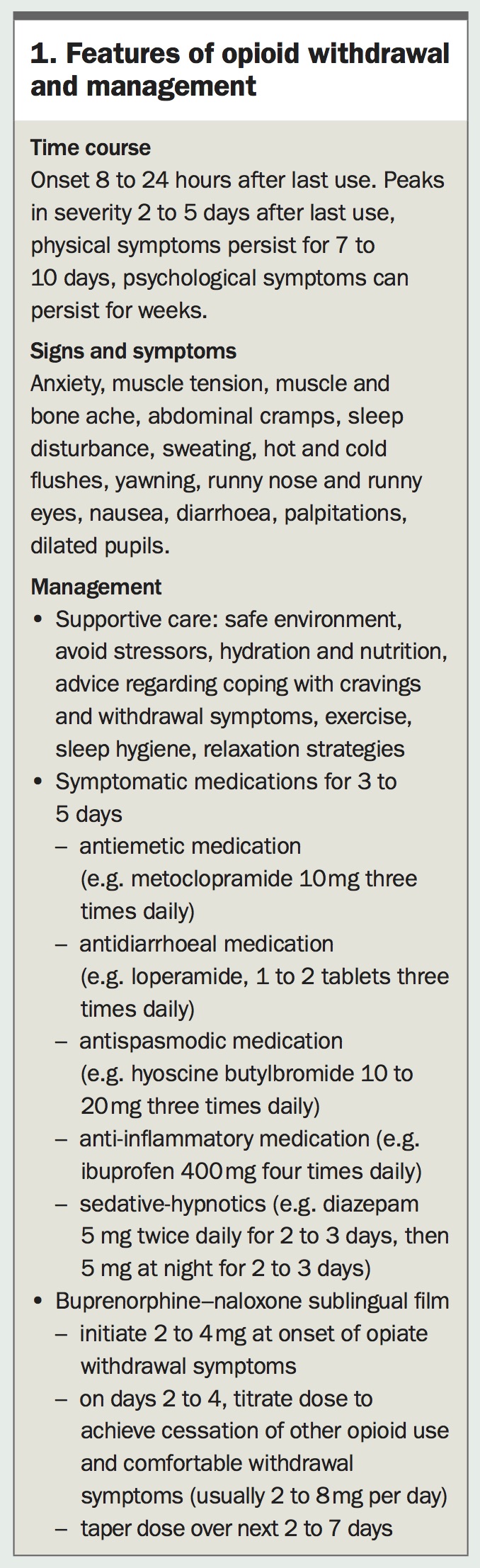
It can be difficult for some patients to understand or accept the diagnosis. Typically the patient experiences worsening of headaches after a period of no (or low-dose) codeine use. In response, the patient resumes codeine use, and experiences headache relief. Symptom relief then allows a reduction in codeine use until the headaches re-emerge, and the cycle repeats. The reduced use of codeine may not be associated with features of opioid withdrawal (Box 1), or obvious withdrawal symptoms may only appear after several days of abstinence.
{kind=link}
The patient may interpret this as ‘the only thing that works is the codeine’, when in fact the codeine is exacerbating the problem. Many patients with MOH see their medication as ‘indispensable’, do not consider themselves as dependent or addicted and can feel offended by any such suggestion.10 MOH occurs with overuse of a range of nonpsychoactive medications with several pathophysiological mechanisms involved – so it is incorrect to associate all patients with opioid-related MOH with opioid withdrawal or dependence.
Consensus opinion suggests the optimal treatment of MOH is cessation of the medication – either abruptly or using tapered dose reductions.11 For opioid-related MOH, an opioid withdrawal syndrome may emerge, peaking in severity during the first two to five days of abstinence. Many patients will experience an increase in headache severity during this time, and it may take one to two months of abstinence for baseline levels to return. A GP reviewing the patient regularly over time will be able to monitor progress and provide reassurance.
Management of opioid withdrawal can usually be achieved in the community, although a minority of patients may benefit from inpatient admission. Key features of opioid withdrawal management are described in Box 1, and involve patient education, supportive care and symptomatic or substitution medication. Although the adrenergic agonist clonidine is effective in opioid withdrawal symptoms, the history of hypotension in this patient would preclude its use. Patients not coping with abrupt opioid cessation may benefit from a tapered course (e.g. five to 10 days) of a long-acting opioid such as buprenorphine–naloxone. Guidelines are available and consultation with a relevant specialist or drug and alcohol service is recommended.12,13
There may be a role for prophylactic treatment of other underlying headache conditions (e.g. migraine) where this is identified, although it remains unclear whether this should be initiated during or after drug withdrawal. Management of other medical, psychiatric and social comorbidities may also be required. An important aim is to restructure the patient’s approach from ‘have pain – take tablet’ to better ways of preventing and managing headache. Patients may benefit from referral to a counsellor or multidisciplinary pain teams to reinforce these behavioural approaches.
Longer-term outcomes with MOH suggest that most (often reported at about 70%) of patients do well after ceasing their analgesic use, although 20 to 40% relapse, generally within the first year.14
Assessment and management of possible opioid dependence
It is not possible from the available information to make a diagnosis of opioid dependence and, indeed, the diagnosis of dependence in the context of opioid analgesic use is often complex. Although the defining characteristic of opioid dependence is diminished control over the use of opioids and persistent use despite harms, this is complicated when the opioid is also used therapeutically. The mere presence of withdrawal or tolerance does not infer dependence, and ‘persistent use despite harms’ with a medication is usually termed in other areas of medicine as ‘tolerating the side effect’. Without further evidence, such as a history of regular codeine use unrelated to headaches (e.g. for intoxication, coping with stress), history of other opioid use (e.g. illicit use) or related harms (e.g. impaired social and occupational functioning), a diagnosis of codeine dependence in this patient should be avoided. This may change over time and, in particular, the inability of the patient to stop codeine use or repeated relapses after periods of abstinence may suggest a diagnosis of dependence.
A diagnosis of opioid dependence indicates an alternative management approach is necessary. Although opioid medication cessation may be an effective approach for managing MOH, the evidence regarding opioid dependence (pharmaceutical and illicit source) indicates withdrawal management alone to be ineffective, with high rates of relapse and poor patient outcomes. The most effective treatment approach is longer-term opioid agonist treatment with buprenorphine–naloxone or methadone, in conjunction with psychosocial interventions (counselling, case management) and management of comorbidities.
For Jason, longer-term opioid treatment may be warranted if he was unable to cease codeine use or repeatedly relapsed to codeine or other opioid use after periods of abstinence. Higher-dose sublingual buprenorphine–naloxone can be a useful medication both for opioid withdrawal or longer-term treatment. In patients not coping with codeine cessation or symptomatic medications, it is worth considering a trial of buprenorphine–naloxone for withdrawal, which may transition to longer-term buprenorphine–naloxone treatment if the patient is unable to achieve longer-term -abstinence. Detailed and summary clinical guidelines are available.12,13
Medicinal cannabis for this patient
There is evidence of cannabis being used for thousands of years in treating headaches, and contemporary surveys of medical cannabis users suggest that headache is a common reason for medical cannabis use. Furthermore, there is increasing understanding of the role of the endocannabinoid system in moderating headaches, with preclinical research highlighting a number of pathophysiological mechanisms.15
Although several systematic reviews conclude that tetrahydrocannabinol (THC)-based medicines can have a modest beneficial effect in treating chronic pain conditions,16,17 there are few well-conducted studies regarding chronic headache. One randomised double-blind, cross-over study compared eight-week courses of oral nabilone (a synthetic THC) with ibuprofen in 30 patients with MOH, with nabilone resulting in significantly greater reductions in pain intensity, daily analgesic intake, medication dependence and quality of life. Although promising, further research is required.18
Given the limited clinical evidence, and the absence of any registered medical -cannabis products in Australia for this indication, medical cannabis remains a second-line treatment approach for patients in whom conventional treatment is ineffective. Patients and clinicians should also consider the risks of medical cannabis use, including common side effects (e.g. lethargy, anxiety, dry mouth) and the potential for developing cannabis dependence – estimated to occur in approximately 10% of long-term users.
Nabiximols (a combination of plant-extracted THC and cannabidiol in an oromucosal spray) is the only licensed medical cannabis medicine in Australia. All other products can only be accessed as unlicensed medicines using the Special Access Scheme (or less commonly Authorised Prescriber or clinical trial pathways), requiring approval from the TGA. Following TGA approval, doctors must also obtain permission from local state health departments to prescribe any THC-based medicine as it is a Schedule 8 drug. In practice, the procedures remain cumbersome and there has been minimal uptake across Australia. Furthermore, as unlicensed medicines, there is no PBS subsidy, and many patients find the cost of medical cannabis products prohibitive.
Clinicians interested in pursuing medical cannabis are directed to the TGA website, including recent guidance for clinicians (www.tga.gov.au/access-medicinal-cannabis-products) and patients (www.tga.gov.au/publication/guidance-use-medicinal-cannabis-australia-patient-information).
Commentary from a neurologist
By Richard Stark
It is important to establish a diagnosis and then produce a rational management plan based on that. Vital points need to be clarified. These include the duration and evolution of the headache pattern, associated clinical features, the frequency of the headaches and how many days of treatment is required. From the case scenario, headache requiring some treatment may be present every day, but some days are worse than others; however, this needs to be confirmed. In most such cases, the examination is normal, but it should be carried out to help exclude sinister underlying pathology.
Diagnostic strategy
The strategy behind the diagnostic process includes the steps outlined below.
Is this a primary headache disorder or is it secondary to some tangible cause?
The list of possible causes of headache is long, and most neurologists have in mind some red flags that point to a sinister pathology. One popular mnemonic for these is SNOOP-4 (Box 2).
{kind=link}
Is this an episodic or chronic daily headache pattern? Are the headaches brief or prolonged?
The current classifications distinguish between headaches occurring more than 15 days a month and those occurring less often. This might seem arbitrary, but there does seem to be some difference in the way headache disorders behave and respond to various treatments when present more than 15 days per month. Therefore an accurate history of headache frequency and treatment use is needed (having the patient do a headache diary, listing days with headache and what treatment was taken is better still).
In most cases of frequent headache, the headache persists for more than four hours. If it is briefer, some unusual headache disorders should be considered. For example, cluster headache will produce excruciating, strictly unilateral ocular pain lasting 30 to 90 minutes and then resolve.
Which primary headache disorder is present?
Most patients with chronic daily headache and no secondary cause have chronic migraine, but other disorders such as hemicrania continua, new daily persistent headache and chronic tension type headache will be recognised by taking a careful history (Flowchart).
Is there medication overuse?
MOH is now recognised to be a superimposed complication of an underlying headache disorder, not a separate condition. Most patients develop MOH from taking increasing amounts of medication to deal with a headache pattern that was originally episodic. The condition then evolves or transforms into a chronic daily headache pattern and in many cases the overuse of medication is a major factor in this transformation. To diagnose MOH, a clear history of the frequency of medication use is required.
The formal definitions of medication overuse in MOH are:
- combination analgesics (with codeine) more than 10 days per month
- triptans, ergots more than 10 days per month (ergots are not available in commercial products but can be obtained from compounding pharmacies)
- simple analgesics more than 15 days per month.
The rationale for these definitions relates to the notion that if the defined frequencies are exceeded, the medication use itself induces a more frequent headache pattern. In the case of codeine, opiate receptors habituate so that when codeine is not taken a withdrawal syndrome develops. In a person prone to migraine, the first symptom of this is recurrence of headache and this naturally responds best (in the short term) to more codeine. But in the longer term this perpetuates the habituation process.
Are there lifestyle factors contributing to the presentation that can be remedied?
These lifestyle factors would include alcohol abuse, disturbed sleep patterns, stress and dietary factors.
What is Jason’s diagnosis?
The case scenario does not permit a definite diagnosis, but:
- there is nothing presented to suggest a secondary cause
- the headaches are probably present daily (they get worse if he stops taking codeine)
- the most likely primary headache diagnosis is migraine – it is the most common cause of disabling headaches and the family history provides some support for the diagnosis. However, one should ask directly about clear-cut features of migraine (e.g. nausea, photophobia, phonophobia and throbbing quality of pain) if they are not volunteered. On the brief history provided chronic tension type headache is possible, but in practice careful history taking (ideally supplemented by a headache diary) confirms a diagnosis of chronic migraine in most patients of this type.
- MOH is very likely but should be confirmed by counting days per month of codeine use.
Thus, the most likely diagnosis is chronic migraine complicated by MOH.
What are Jason’s treatment options (assuming the diagnosis of chronic migraine complicated by MOH)?
His migraine should be treated, with the following steps outlined below.
- Manage any modifiable triggers. This may be hard as stress and hot environments are difficult to avoid in his occupation.
- Treat headaches effectively when they occur (keeping the risk of MOH in mind). In patients with frequent migraine, a stepped approach is often required using triptans for severe attacks and NSAIDs for milder ones. Five different triptans are available, providing a range of options: if one produces insufficient benefit or troublesome side effects another member of the class may be more suitable. Intranasal or wafer formulations may be helpful in patients who do not absorb tablets well during a migraine attack due to associated gastric stasis.
- Prophylactic medication should be used. There are many options and the choice for an individual will often depend on comorbidities. For example, antihypertensive agents such as propranolol or candesartan (off-label use for migraine) may be less attractive in a patient with symptomatic hypotension such as Jason. Overweight patients should avoid pizotifen. Amitriptyline, sodium valproate (off-label use for migraine) and topiramate might be considered. Botulinum toxin type A is effective for chronic migraine and is PBS funded (authority required) in patients who have had an inadequate response, intolerance or a contraindication to at least three prophylactic migraine medications and in whom MOH is appropriately managed. Nonpharmacological methods of migraine prophylaxis such as neurostimulation devices have some evidence of benefit.
At the same time, MOH should be addressed, as outlined below.
- If Jason’s use of codeine had been intermittent (less than 10 days a month), it could simply be replaced by other agents such a potent triptan.
- If, as seems likely, his codeine use is frequent, a detoxification strategy will be required. He will need to refrain from using codeine long enough for his opioid receptors and other elements of the pain pathways to reset. This will take two to four weeks and during this time there will be a significant withdrawal headache to manage. This process needs commitment and fortitude from the patient and support from their doctor. It requires the following approach.
– The patient must understand the process and commit to it, which most patients will readily do. They are taking codeine as a means of dealing with intolerable headache – there is no recreational element to their opioid use and they must be told explicitly that their doctor understands this. Patients are often delighted to cease codeine if their headaches can be managed effectively without it.
– Management of the withdrawal headache, often done in an outpatient setting. There are various protocols using high-dose NSAIDs or a course of prednisolone. However, the patient is likely to be unable to work or perform routine household responsibilities for the first week at least (trying to continue work during this time often results in failure).
– Inpatient detoxification using techniques such as intravenous dihydroergotamine or lignocaine for headache control (off-label uses) in some patients.
– A clear plan for aggressive migraine management (without codeine) after the withdrawal process is completed.
Summary
A clear diagnosis of the cause of disabling headache is a vital first step. The most likely cause is migraine. A wide range of highly effective therapies for the prevention and acute treatment of migraine are available. Opioids are rarely required. MOH complicating migraine must be recognised and addressed. It is easier to avoid than to treat, but effective treatment strategies exist. PMT
COMPETING INTERESTS: Dr McCoy has received personal fees from Mundipharma and Sequiris. Professor Lintzeris is an advisory board member for Mundipharma and Indivior, and has received research grants from Indivior. Associate Professor Stark has received personal fees from Allergan, Novartis, Teva, SciGen and InVivo Academy.