Cluster headache. How to ‘break the bout’ early

Headache
Pain
Cluster headache is an extremely painful and disabling condition. Often there is a significant delay to diagnosis. Medical interventions can shorten or ameliorate the intensity of discomfort during an attack. The best management strategy is to terminate a bout early.
- The diagnosis of cluster headache should not be missed. Other diagnoses such as paroxysmal hemicrania may need to be actively excluded.
- Management strategies for cluster headache are often effective.
- Patients should be referred to a neurologist if the diagnosis is in doubt or if initial management strategies have failed.
- Several new treatment modalities will become available soon for treatment-resistant patients.
Migraine occurs in 15% of the population regardless of location around the world, and accounts for the most troublesome headache presentations.1 Cluster headache is not as common as migraine but is by no means rare, occurring in about one in 1000 people.2 It is a disabling condition, with patients describing the pain as more severe than childbirth or breaking a bone. It is important for clinicians to recognise the possibility of the condition, proceed through logical steps to confirm the diagnosis and then treat. Typically, patients will have gone many years without a diagnosis but once diagnosed many respond well to first-line strategies. Perhaps as a result of the level of disability and suffering associated with this condition, patients are particularly grateful for an accurate assessment and appropriate treatment strategy.
Clinical features
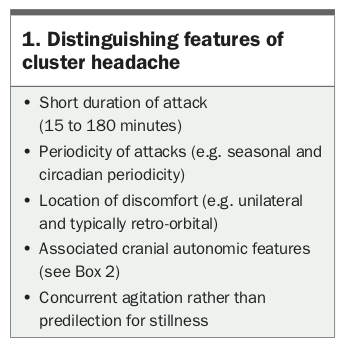
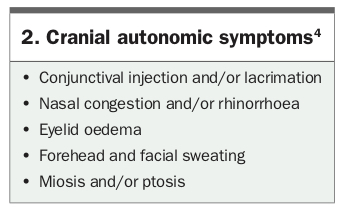
Cluster headache consists of a very severe discomfort that is unilateral and typically retro-orbital. Pain is usually characterised as a stabbing sensation but alternative descriptors can be vivid, such as a ‘hot poker in the eye’.3 The duration of the attack lasts from 15 to 180 minutes. Other distinguishing features of cluster headache are listed in Box 1. There should also be at least one ipsilateral cranial autonomic symptom or sign, such as rhinorrhoea (Box 2).4
{kind=link}
{kind=link}
Most patients have attacks at set times in the day within particular weeks of the year at regular intervals. The weeks or months within which attacks occur are described as a bout. Patients who never have respite, who are always within a bout, are described as having chronic cluster headache. They make up about 10% of patients with cluster headache. Patients with episodic cluster headache tend to have bouts that run for four to six weeks, most commonly around the equinox (i.e. when the rate of change of the length of the day is greatest).
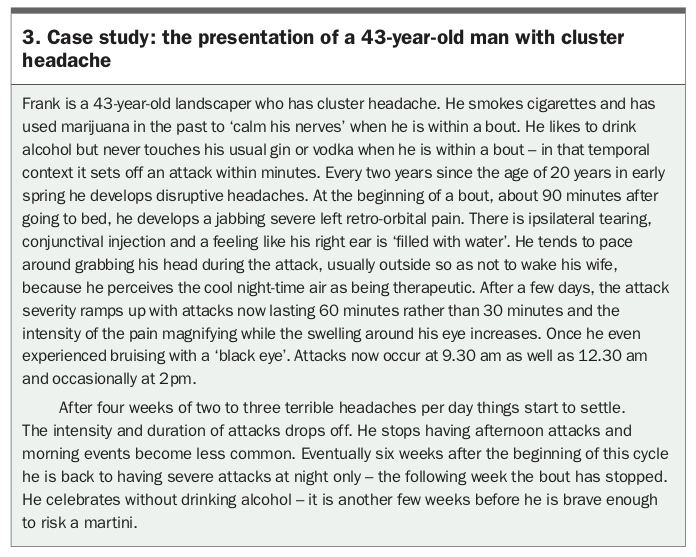
Patients are more commonly men, and often have comorbid substance abuse and psychopathology (Box 3 outlines a case presentation of a man with cluster headache). Enquiries regarding sleep, mood, suicidal ideation and use of drugs should be actively made.
{kind=link}
Trigeminal autonomic cephalalgias
The trigeminal autonomic cephalalgias (TACs) form a group of short-lasting headaches that are associated with cranial autonomic symptoms. The most studied and best known TAC in clinical practice is cluster headache. The other syndromes within this group are:
- hemicrania continua
- short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache with cranial autonomic features (SUNA)
- paroxysmal hemicrania.5
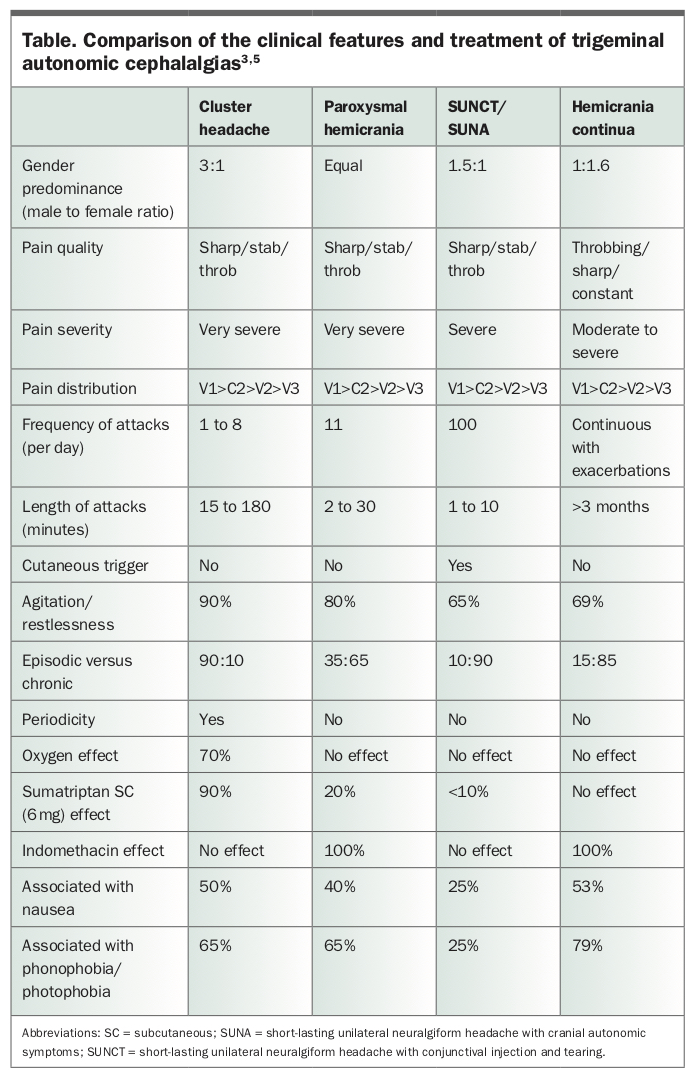
There is some overlap of phenomenology between TAC subtypes, particularly the presence of cranial autonomic features. Timing and treatment response define each different TAC (Table). The main differential diagnosis of cluster headache is paroxysmal hemicrania. In this condition, attacks tend to be shorter and less predictable in timing than cluster headache, and use of indomethacin completely eliminates symptoms. Most patients will require an indomethacin trial early on to eliminate paroxysmal hemicrania as a differential diagnosis.
{kind=link}
Cranial autonomic symptoms represent activation of parasympathetic output mediated by the seventh cranial nerve via the sphenopalatine ganglion and/or interruption of sympathetic output ipsilateral to pain. The physiology is established, easy to understand and important to remember.3,5
Masqueraders
Patients with migraine can often have a poor sense of how long their headaches last, sometimes only reporting the particularly excruciating elements and forgetting to report the more moderate discomfort. A thorough set of questions about headache duration and other migrainous features are usually adequate to differentiate cluster headache from migraine. However, migraine can occur comorbidly with cluster headache, whereas migrainous symptoms such as photophobia can accompany a cluster attack.
Two-thirds of patients with migraine have either unilateral or bilateral cranial autonomic features (Box 2), often ipsilateral to discomfort. The presence of these symptoms does not imply a TAC. The diagnosis of ‘cluster migraine’, still in existence in the general and medical community, has no place in headache nosology. Some practitioners use this terminology to imply periodicity. However, patients with primary headache, such as migraine, often manifest headache at night, or for discrete periods of days, or every few months for a few weeks. Some doctors use the term to imply cranial autonomic features such as aural fullness or periorbital oedema, which is also confusing. It is worth noting that 90% of ‘sinus’ headache diagnosed in the community is migraine with the prominent cranial autonomic symptom of nasal fullness.6 Amoxicillin and clavulanic acid do not help migraine, even if headaches seem to subside. It is the natural history of headaches to wax and wane.
If the headaches are not severe, tend to last for hours, lack periodicity and lack associated cranial autonomic features and/or agitation, then it is not cluster headache.
Many people with migraine experience ice-pick pains – primary stabbing headache.4 These can occur anywhere in the head. As they are sharp, painful and intermittent, this can mislead practitioners into invoking a diagnosis of TAC.
Trigeminal neuralgia is often considered in a patient with short-lasting pains in the face or head. In contrast to cluster headache, trigeminal neuralgia tends to last for seconds not minutes. Lancinating discomfort tends to occur in V2 or V3, can be triggered by stimuli such as talking or touching the face, and is usually followed by a refractory period of seconds to minutes where an attack is not triggered, allowing the patient to eat or talk.
Pathophysiology, imaging and endocrine changes
The remarkable seasonal periodicity of bouts and circadian periodicity of cluster headache attacks implies an unfortunate chronobiology. As the master clock in the body resides in the suprachiasmatic nucleus in the hypothalamus, the longstanding assumption over decades is that the headache is caused by derangement within this small midline structure of the brain. PET studies have demonstrated increased hypothalamic metabolism in induced and spontaneous cluster headache attacks.3 Endocrine changes implying hypothalamic dysfunction have been recorded. Deep brain stimulation of the hypothalamus has been performed in about 50 people worldwide leading to headache remission in more than 50% – proof of the central role of the hypothalamus in the aberrant circuitry driving the phenomenology.7 Some of the brain structures that mediate cranial discomfort in cluster headache, such as the trigeminal nucleus caudalis, are also involved in other primary headache conditions such as migraine.
When first diagnosed with a TAC such as cluster headache, a secondary cause of headache requires exclusion. A history consistent with previous trauma or pituitary dysfunction should be sought. Although most patients with cluster headache do not have pituitary abnormality, primary headaches such as the TACs are relatively preponderant in patients with pituitary micro- and macroadenoma.8 Mandatory investigations therefore include an MRI of the brain and pituitary (sella views), as well as a serum anterior pituitary screen.
Management
Patients tend to come up with elaborate behavioural strategies to cope with the severity of a headache ictus including cold compresses, eating or snorting chilli, menthol wipes over the forehead, pressing into the eyeball, squashing the back of the head against a wall, dunking the head in ice water and inducing a sneeze. Medical interventions can shorten or ameliorate the intensity of discomfort during an acute attack. The best strategy is to get ahead of the curve and reduce attacks by terminating a bout early.
Acute management
The best acute medication for cluster headache is subcutaneous injection of sumatriptan 6mg, which unfortunately is not on the PBS. Regular use is prohibitively expensive for most people. The intranasal formulation is often useful but tends to take longer to act and is less reliable in its efficacy. Most patients tend to use both at different times. Oral triptans are of limited use in this condition.
High-flow oxygen therapy (12 to 15 L per minute via a non-rebreather mask) aborts an attack within minutes for most patients. Although the therapy is not government funded it is not cost prohibitive. One month’s supply is comparable in cost to about three subcutaneous sumatriptan doses. Patients require a prescription or letter to present to their local oxygen supply company who provide both the oxygen tank and appropriate peripherals. If the patient smokes, this treatment is not recommended due to the risk of burns. Most experienced patients use a large rented oxygen tank at home when they are within a bout and use triptans when they are away from home. Occasionally patients will pay for a small portable tank as well, but cost soon becomes an issue. In the context of a bout, patients are often reticent to plan social events or trips, and they curtail or regulate work activities.
Preventive management
The ideal intervention is to ‘break the bout’ at onset with use of a greater occipital nerve (GON) block. Steroid and local anaesthetic – for example, 80 mg methylprednisolone and 3 mL of 1% lignocaine – infiltrated in and around the GON ipsilateral to the pain will stop the bout in its tracks in many patients. This intervention is simple to learn and perform, and a useful skill for GPs to acquire, particularly in regional Australia. The advantage of referring the patient to a neurologist is that they can also flesh out the diagnosis and spend some time explaining the condition to the patient, and answering pertinent questions, especially as this group of patients relies all too much on online forums. GPs are encouraged to learn the useful skill of a GON injection.
If this strategy is unavailable, unsuccessful or not preferred by the patient, the next intervention to try is a short course of oral corticosteroids (e.g. start at 75 mg and wean gradually over two weeks) with or without a gradually escalating use of verapamil (off-label use; doses as high as 500 mg daily can sometimes be used). A baseline ECG must be completed and the PR interval watched as heart block can occur and progress over time even in the context of stable dosing.
Patients may have already tried these first-line strategies and not responded. There are a host of other alternative preventives such as melatonin (up to 15 mg each night), lithium, topiramate and inpatient options such as dihydroergotamine (all off label for treating cluster headache). Other interventions such as the occipital nerve stimulator can occasionally be appropriate. A neurologist should be involved in care if initial strategies have been ineffective.
Future strategies
Future strategies for cluster headache include use of a hand-held vagus nerve stimulator device, available from the US, which has an evidence base in terms of safety and efficacy as an acute and preventive treatment; however, the downside is cost.9 Sphenopalatine ganglion stimulation, used in the US and Europe, will also be useful for patients with refractory cluster headache when it becomes available. Trials of calcitonin gene-related peptide are ongoing and may provide a novel therapeutic avenue. Galcanezumab, one iteration of this class of medication and as yet unavailable in Australia, was recently approved by the FDA for use in episodic cluster headache.10
Conclusion
Cluster headache is an under-recognised painful condition that causes significant disability in our community. Delay to diagnosis is significant and usually takes years. Interventions are usually extremely helpful. Decreasing morbidity in this patient population is very satisfying for both the patient and health carer. PMT