Fibromyalgia syndrome: ‘a dose of the flu that lasts forever’
Fibromyalgia
Pain
Fibromyalgia syndrome results in widespread pain and other symptoms related largely to dysregulation of the neuroimmune system. It is often described by patients as ‘feeling like a never-ending dose of the flu’. It can be regarded as a chronic stress-or-sickness response and should be managed using a multimodal approach.
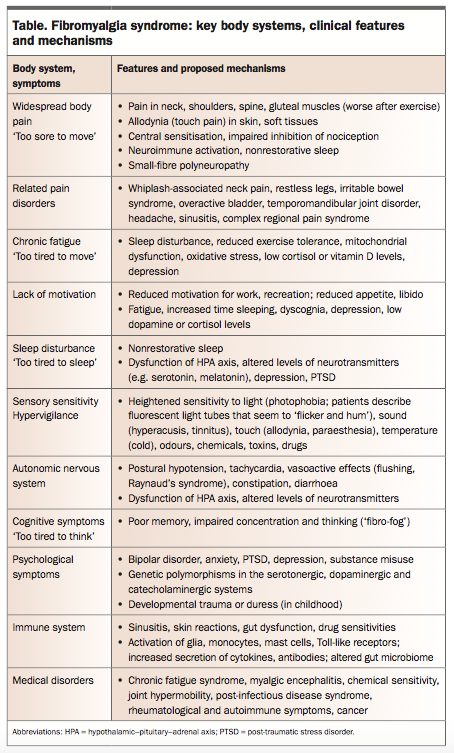
- People with fibromyalgia syndrome (FMS) present with chronic widespread pain, fatigue, sleep disturbance, sensory sensitivity and psychocognitive dysfunction.
- In FMS there is evidence of psychoneuroimmune, cortical and endocrine dysfunction and in some cases widespread small-fibre polyneuropathy.
- Illness, stress, duress and trauma are common triggers of FMS, and there is a strong link to mood and anxiety disorders.
- The whole person with FMS should be managed using a biomedical psychosocial approach.
Picture credit: © Science Source/Jim Dowdalls/Diomedia.com
Case scenario
A 43-year-old woman presents with an 18-month history of widespread body and neck pain, chronic fatigue, sleep disturbance and altered mood after a whiplash-associated neck injury from a motor vehicle accident. She has flashbacks and dreams of the crash, has lost her job and is involved in legal action for compensation. She feels like she has a ‘dose of the flu that is lasting forever’.
{kind=link}
Diagnostic criteria for FMS are based on the number of body regions affected by pain and the severity of systemic symptoms.1 FMS affects up to 8% of the population, most commonly women between 30 and 60 years of age.2,3 About 30% of patients with a localised chronic pain disorder develop FMS. The incidence of FMS is increased in patients with bipolar disorder, anxiety, depression or a family history of FMS.3
Proposed mechanisms
FMS may be considered to be part of a spectrum of systemic stress disorders with similar mechanisms and aetiologies. These disorders include chronic fatigue syndrome, myalgic encephalitis, chemical sensitivity syndrome and Gulf War syndrome. The term fibromyalgia (meaning painful fibromuscular tissues) is a historically outdated term from a time when the condition was considered to be a muscle disorder.1
Stress and allostatic load
Organisms, including humans, have evolved systems to deal with threats against their viability. These threats are known as ‘stressors’ – that is, any factor that alters normal homeostasis (functional balance). Stressors can apply to the organism as a whole or to a specific organ system. The cumulative effect of stressors on homeostasis and tissue viability is known as allostatic load.2,3
An organism can generate a set of defensive stress responses to counter allostatic load. Pain, fear, nausea and itch are examples of targeted stress responses that protect an organism from tissue damage.4 The acute stress response (‘fight or flight’) is the best-known rapid defence system that protects an organism from imminent threat.2-4
An organism can only maintain the energy-demanding acute stress response for a few hours at a time. If exposed to prolonged or overwhelming stress, the organism will instead initiate a chronic stress response, known as the sickness response.5 Organisms, including humans, can accumulate an allostatic load over a lifetime. After stress exposure, the organism incurs an ‘allostatic debt’, because homeostasis never fully returns to pre-stress levels. As a consequence, less allostatic load is required to trigger a subsequent sickness response.3-5
FMS as a chronic stress-or-sickness response
FMS may be thought of as a whole-body chronic stress-or-sickness response, triggered by a range of physiological or psychological stressors (biomedical, psychosocial and environmental). Common stressors include trauma or injury (e.g. whiplash neck injury), illness (e.g. cancer, arthritis or influenza) and adverse life events (e.g. childhood duress or post-traumatic stress disorder [PTSD]). It does not matter if a stressor is psychological, environmental or pathological; the body will respond in the same way – with an acute or chronic stress response.4
Visser and Davies proposed that the sickness response is part of a whole-body defence system (the ‘threat matrix’), which generates polymodal responses (pain, nausea, experiences of noxious heat or cold, itch, panic, dyspnoea, fatigue, dissociative states) in response to any threat to a person’s viability.4
The sickness response and its clinical manifestation, FMS, are characterised by significant changes in the body’s neurological, immune and endocrine systems. These changes are associated with widespread body pain and other symptoms, such as chronic fatigue, sleep disturbance, heightened responses to sensory stimuli (e.g. cold, light and sound), lack of energy and motivation, difficulty thinking, poor memory, depression, anxiety and reduced appetite and libido.3
Many people will have experienced the feeling of the sickness response and FMS when they have had a cold or flu. The sickness response could be described as a ‘hibernation’ response, to conserve energy and re-establish homeostasis, as an adaptation to stress. This is clearly an adaptive response when we are fighting an infection, and the response only lasts a few days. However, if a person is exposed to overwhelming or long-term stress, the sickness response may persist for a prolonged period. It then becomes maladaptive and may manifest clinically as FMS.
Pathophysiology
Neuroimmune dysfunction
The neuroimmune system is activated with glia, macrophages, monocytes, mast cells and neurons, which produce mediators (cytokines, antibodies and neuropeptides, such as substance P) that contribute to the chronic sickness response.2-6 Toll-like receptors (TLRs) play a key role in regulating the innate immune system. Pilot studies have shown that TLR-blocking agents such as naltrexone and melatonin may have a clinical effect in FMS and inflammatory diseases such as Crohn’s disease, but these treatments are still considered experimental.6
Central versus peripheral nervous system effects
In FMS, the body’s nociceptive system becomes sensitised and responses are amplified, in a process known as central sensitisation. Inhibitory nociceptive systems also become less effective. Patients with FMS show reduced tolerance to noxious stimuli and heightened sensitivity to non-noxious stimuli, with altered neuroprocessing of touch, pressure, temperature, sound and chemical stimuli.7
FMS is largely a CNS neuroprocessing disorder. It is characterised by widespread pain reflecting cutaneous, somatic and visceral allodynia. Wolfe’s classic tender points for fibromyalgia represent reproducible sites of pressure-evoked pain.8 However, the peripheral nervous system may also be involved, with recent studies suggesting that at least 30% of patients with FMS have small-fibre sensory polyneuropathy which may cause neuropathic pain.9
Cortical and autonomic changes
Functional neuroimaging has shown cortical and thalamic changes in patients with FMS, and there is evidence of dopaminergic neurotransmitter dysfunction in the limbic system. There is also evidence of significant autonomic nervous system dysfunction (postural hypotension and altered heart rate variability, including postural orthostatic tachycardia syndrome) and an impaired sympathetic response to stress.3 Sleep disturbance and hypothalamic dysfunction are also key features of the sickness response and FMS. These features are associated with electroencephalographic changes and sleep-disordered breathing.3
Endocrine dysfunction
Patients who have FMS show impaired hypothalamic–pituitary–adrenal axis responses to stress. There are changes to the levels of some hormones (growth hormone and cortisol) and of various neurotransmitters which control nociception, mood and sleep (substance P, noradrenaline, serotonin, melatonin, nerve growth factor and dynorphin).3
Altered gut microbiome and free radical production
FMS, and related conditions such as chronic fatigue syndrome, may be associated with dysfunction of the gut–brain axis and the microbiome. Altered mitochondrial energy processing, particularly in skeletal muscle, and the overproduction of oxygen and nitrogen free-radical species may also be associated with these syndromes.10
Psychosocial factors
There is a strong correlation between FMS and mood disorders among patients and their families. The strongest correlations are with bipolar disorder, obsessive–compulsive disorder and PTSD.11 FMS has been shown to be associated with genetic polymorphisms in the serotonergic, dopaminergic and catecholaminergic systems of pain transmission and processing, which are also implicated in mood disorders.12
The incidence of stressful life events in childhood or adolescence, particularly before the onset of symptoms, is significantly higher in patients with FMS compared with healthy controls and people with rheumatoid arthritis.11 For a patient with FMS, their psychosocial stressor load and their use of healthcare resources are also significantly greater if more than 20% of their body surface area is affected by pain, as drawn on a body diagram.13
The links between psychological stress and FMS are likely to be multifactorial but there are certainly neurobiological contributors. Patients with hypothalamic–pituitary–adrenal axis dysfunction (impaired dexamethasone suppression and abnormal diurnal cortisol levels) are at significantly increased risk of developing chronic widespread pain.14 Chronic psychological stress generates cytokines which (via neuroimmune mechanisms) may produce anxiety, depressed mood and widespread pain; the hallmarks of FMS.15
Conclusion
The patient in the case scenario is representative of the most common population in which FMS occurs (women between 30 and 60 years of age). She reports key symptoms (pain, fatigue and neurosensory dysfunction) and was exposed to a significant allostatic load. Her cumulative stressors include a motor vehicle accident, chronic pain and illness, PTSD, and social, legal and financial issues. She also reports two of the most prevalent clinical conditions associated with FMS, whiplash-associated neck pain and PTSD. Finally, the description of how she feels, as if she has an ongoing dose of the flu, reflects the chronic sickness response her body is mounting to deal with her stressor load.
FMS is a prime example of a complex biomedical, psychosocial and environmental syndrome associated with whole-person physiological and psychocognitive effects. It is largely a chronic sickness response to an allostatic load in a vulnerable person. Therefore, management of patients must reflect the complex aetiology of the condition by using a whole-person, multimodal approach. PMT