The place of interventional pain procedures

Pain
Interventional pain procedures are used for diagnosis and localisation of pain, and are also used for therapeutic purposes. They can be an additional tool to manage pain symptoms and must be considered part of the range of strategies for pain management.
- If the patient has a dominant anatomical pain source, pain procedures can be part of the range of socio psychobiological strategies for pain management.
- Pain medicine physicians are trained to incorporate active behavioural strategies with conventional medical options.
- Pain medicine physicians decide whether pain procedures are suitable and which procedures to perform.
- People with pain should be encouraged to undertake daily walking, simple movements, pacing activities, mindfulness meditation and threat-reduction activities before pain procedures.
- Pain cannot be localised using current imaging techniques, so pain procedures are used to help diagnose anatomical pain sources.
- Therapeutic pain procedures can provide three to12 months of pain reduction, which can provide a therapeutic window for the patient to progress with their active behavioural pain strategies.
- If therapeutic procedures provide the patient with pain relief and the pain then recurs, a repeat procedure will usually provide similar relief if the pain sources are shown to be the same.
Interventional pain procedures are part of an integrated, broader pain management plan. The aim of these procedures is to treat people with chronic pain. They are performed in conjunction with specific rehabilitative interventions and pain education that is taught by doctors, physiotherapists, occupational therapists, chiropractors, exercise physiologists and pain psychologists. These practitioners teach active pain strategies and skills such as coaching for daily walking and activities (pacing), simple movements and stretches, muscle retraining, short-term goal setting, motor-guided imagery, mindfulness, meditation and relaxation. Yoga and Tai Chi are good group-based options for some of these skills and are readily available in the community.
Before considering an interventional pain procedure, the person in pain should be engaged in their own prehabilitation, movements and pacing activities. After the patient assessment, pain options relevant to the individual patient should be discussed. A pain management plan is then agreed on and understood by the patient (and their partner or family members) and the treating medical doctor, and communicated to other relevant healthcare professionals (‘coaches’).
There are individual and societal complexities relating to the person in pain, and pain can have the added complication of many inputs from multiple separate anatomical structures.
Isolation of specific anatomical targets that contribute significantly to a person’s pain can help guide low-risk procedural pain interventions that can provide medium- to long-term relief. These interventions modulate pain with biological reversal of some pain pathways, rather than providing an anatomical ‘fix’. Specifically, the emerging biology of pulsed radiofrequency neurotomies (also known as rhizotomies) shows that these procedures are unique, in that they provide pain relief without causing significant damage to nervous tissue. Animal studies show that modulation of pain transmission in the spinal nerves and spinal cord can be achieved by a range of mechanisms, including modulating gene expression1 and microglial neuro-transmitters.2-4 These concepts are beginning to provide explanations of the biological mechanisms for pulsed radio-frequency modalities for managing pain.
This article presents a simplified version of anatomical pain and how interventional procedures are used. In clinical practice and research, healthcare professionals and patients need to be aware that the clinical reality is not always straightforward. Patients commonly present with more than one pain source, and so it is common for patients to undergo combined procedures.
The definitions of diagnostic and therapeutic interventional pain procedures have previously been discussed and are outlined in the Box.5,6 Here, we will focus on spinal pain because most of our specialist procedural work (about 70 to 90%) is treating spinal pain, with about 5 to 15% of our procedural work being for joint pain and about 5 to 15% being for regional pain. Pain procedures are discussed in two sections; diagnostic procedures and therapeutic procedures.
{kind=link}
Diagnostic procedures
Facet joint injections and medial branch blocks
The only way to confirm if facet joints are contributing to back pain is to perform low-risk diagnostic facet joint injections or medial branch blocks using local anaesthetic (LA). Back pain is common, with 80% of people having a significant episode of back pain during their life. Causative lesions are often not visible when imaging methods such as plain x-ray, MRI, CT or bone scanning are used.7 The preferred current method to establish if spinal pain is coming from facet joints is to perform facet joint injections or medial branch blocks. The facet joints and muscles behind them commonly contribute to lumbar and cervical spinal pain, and less commonly to thoracic spinal pain. Facet joint pain can be localised to the back or can radiate to other parts of the body. Cervical facet joint pain can spread up and over the back of the head or down the arm (but not usually into the fingers). Thoracic facet joint pain can spread around the anterior chest, and lumbar facet joint pain can spread down to the legs (but not usually into the toes).
Facet joint injections and medial branch blocks are performed using LA, with imaging to confirm the position of the needle.8,9 The LA numbs the facet joints and posterior elements (the structures behind the facet joints) for several hours (the block time varies depending on the LA used). If the patient’s pain is reduced by 50 to 70%, a tentative diagnosis can be made that that percentage of pain is coming from the facet joints or posterior elements.
It is often misunderstood that facet joint injections (or medial branch blocks) are performed primarily for diagnosis.10-14 The confusion occurs because some patients also get ongoing relief, which is a ‘bonus’ therapeutic effect. If it can be shown that a significant part of the pain is coming from the facet joints, during the LA phase, without ongoing pain relief resulting, neurotomies (at multiple levels) can be performed, which often provide longer-lasting relief, sometimes for many months.15
Intervertebral disc injections
The only way to confirm which (if any) intervertebral discs are contributing to pain is to perform diagnostic disc injections using LA and imaging (discography). Disc injections are usually at a single disc level, or in some cases at two or three levels. The LA numbs the disc for a few hours. If there is pain provocation of 70%, this may indicate that the disc is a pain source, but the false-positive rates are high for this procedure.16
It is best to maximise use of pain therapies before disc injections because infection in the disc (discitis) after disc injection is more likely and can be more serious than for other spinal pain procedures. The risk of discitis is about one in 100 to one in 1000, even when prophylactic antibiotics are given at the time of the procedure.
Disc injections can be requested by -surgeons before they consider spinal fusion and after more common sources of pain have been excluded.16
Peripheral joint injections
Injections into the sacroiliac joint, shoulder, hip, knee, and hands and feet, using imaging and contrast dye to localise injections, then using corticosteroid and LA, are often diagnostic and therapeutic.17-21 If the corticosteroid does not provide ongoing relief, animal-derived or synthetic hyaluronic acid or platelet-rich plasma are also options to consider.22,23
MRI and high-intensity zones
If pain radiates to the fingers or toes, radicular pain is considered, and an MRI may further delineate the affected anatomical areas. The most common changes associated with spinal pain that are seen with MRI are high-intensity zones (HIZs; annular tears or fissures), which show as white dots on the scan. The HIZs in the posterior disc are a result of inflammation that can lead to inflammatory fluid accumulating in the epidural space, which irritates the nerve where it exits the spine through the foramen, close to the disc. In our pain practice, we call this characteristic white dot the ‘Davies dot of pain’. We have spent the past few decades looking for these white dots and teaching pain registrars, GPs and physiotherapists to look for them, because radiology reports are variable in commenting on them. It is important to note that these white dots look nonthreatening, so giving them a nonthreatening name can help reduce a patient’s concern about anatomical changes. We show the scans to patients because the scans help us explain a person’s pain and thus help them gain a better understanding of their pain and their spine.
These HIZs are only seen on the T2-weighted, or extra short-TI inversion recovery (STIR) films, in which the higher magnetic spin makes fluid such as cerebrospinal fluid (CSF) appear white. Inflammatory fluid in the epidural space can not be identified on MRI scans because it looks the same as CSF on an MRI scan. The inflammatory chemicals irritate the nerves, causing neuralgia (chemical radiculitis). The pain from radiculitis has been described as shooting pain or electric shocks, and it can make the arms or legs feel like they are expanding or ‘exploding’. The skin is often sensitive and painful to touch (allodynia), which is a hallmark of nerve pain (neuralgia or neuropathic pain).
Radiological reports vary in whether comments are made about these small HIZ changes, which appear benign. It is often useful to show the HIZs on scans to patients, because it can help them gain a better understanding of their pain and their spine. Telling patients that the white dots are not tears or fissures, but are signs of the body healing itself through the inflammatory process, can be helpful.
Therapeutic procedures
The aim of therapeutic procedures is to provide pain relief for a few or many months.
Neurotomy
Neurotomy, a common therapeutic procedure, requires a precisely placed needle or probe over the anatomical path of the sensory nerve from the established pain source. There has been some development of devices and modes, for example, the introduction of cooled thermal radiofrequency.
Pain messages are interrupted by targeting the nerve(s) that supply the pain source. The following percutaneous procedures do not physically cut the nerve; rather, they alter nerve conduction. Nerve conduction can be interrupted using different modalities, -needles and probes, as follows.
- Pulsed radiofrequency neurotomy (PRFN) uses neuromodulation to reduce pain messages. This does not destroy the functionality of the nerve and does not inhibit multifidus muscle contractions. Pain flares are uncommon.
- Cryotherapy neurotomy involves freezing the nerve and is commonly used if patients have a pacemaker. It reduces the functionality of the nerve for a variable period of time. It results in inhibition of multifidus muscle contractions for several weeks and pain flares are uncommon.
- Continous (thermal) radiofrequency neurotomy (CRFN) causes a thermal burn in the tissues. It is also known as radiofrequency ablation, as it destroys the functionality of the nerve for a variable period of time. CRFN inhibits multifidus muscle contractions for -several months and can cause pain flares.
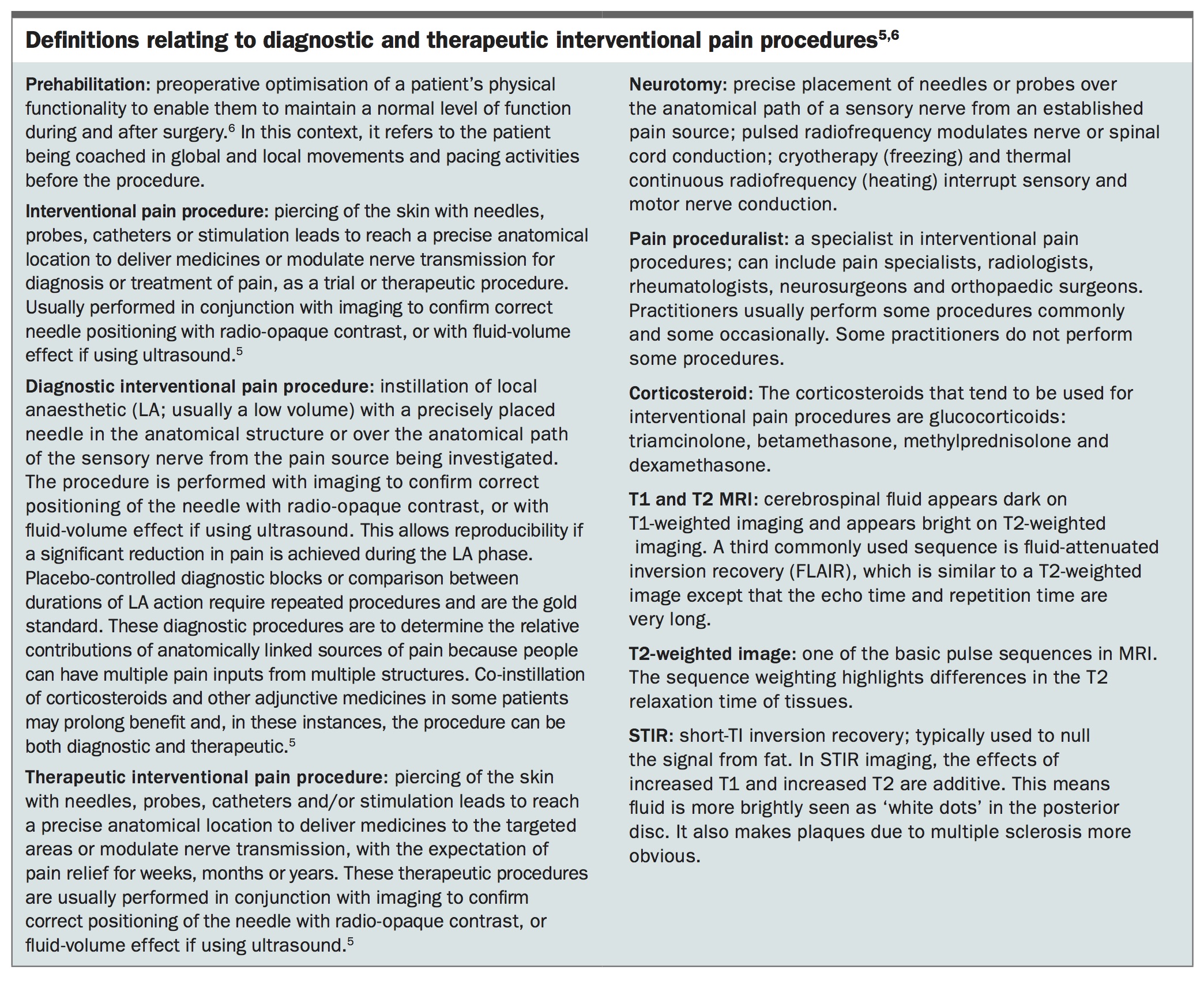
- Probes with expanding tines or a split probe tip enhance radiofrequency and increase the area of modulation (in PRFN) or ablation (in CRFN) (Figure 1).
- For facet joint pain (posterior element pain), pain proceduralists perform neurotomies targeting the medial branches of the dorsal rami nerves that supply the painful facet joints.14,24 Intra-articular PRFN can also be used for small joints.
{kind=link}
Joint denervation
Pulsed radiofrequency modulation is useful when injections do not provide relief from peripheral joint pain. Examples of this are the suprascapular nerve of the shoulder, the geniculate and saphenous nerves of the knee and the obturator nerve of the hip.
Epidurograms and epidural corticosteroid injections
It is a key point that clinical examination (rather than radiological reports) is the best indicator of the symptomatic nerve root, followed by re-checking of the T2 MRI images for central or foraminal white dots. An epidurogram is used to corroborate pain symptom levels.
Disc bulges, protrusions or extrusions causing neuralgia also respond to targeted epidural corticosteroid injections and anti-tissue necrosis factor antagonists.25-29
Many people have a mixed pain pattern with a posterior element (facet joint and multifidus muscle) and radicular pain. Therefore, there can be many pain sources. In these cases, combined procedures can be appropriate, such as PRFN and caudal-entry epidurograms with transforaminal epidural corticosteroid injections, based on the epidurogram (Figure 2).
{kind=link}
Peripheral electrical nerve stimulation
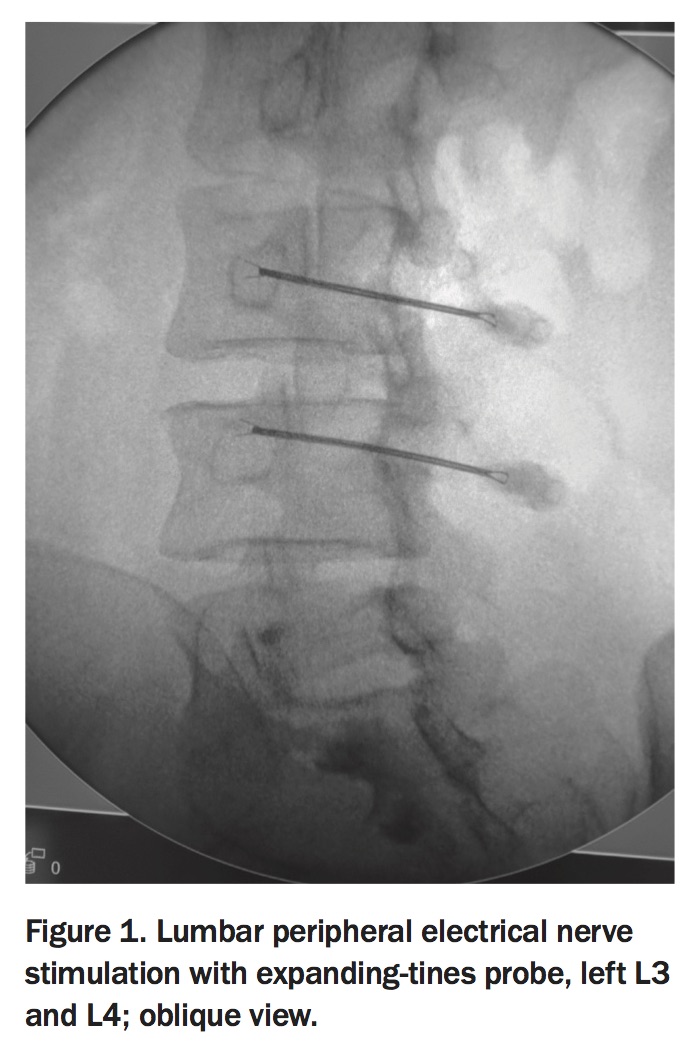
Peripheral electrical nerve stimulation (PENS) probes are used selectively to stimulate peripheral nerves for the relief of chronic neuropathic pain. PENS is used along an identified nerve or in an area of neuropathic pain, using pulsed radio frequency for 25 minutes in the recovery room after the operation to place the probes (Figure 3).30,31 A short electrically conductive probe is inserted either alongside the peripheral nerve (peripheral nerve stimulation) or placed in a painful area that may not be associated with a named peripheral nerve (peripheral nerve field stimulation) with ultrasound to ensure it is positioned correctly.
{kind=link}
The NeuroStimulator PENS therapy electrical generator is provided free on loan, and is reusable. The PENS probes are sterile for single use with costs comparable to probes used for neurotomies. Typically either one or two probes are used for each patient. If the pain returns, PENS therapy can be repeated and an implanted device can be considered; however, these are costly. Lower-cost deployable probes with external radio frequency transmitters may become available in Australia later in 2018.
Stimulators
Neuromodulation is a rapidly expanding area of research, with the development of paraesthesia-free stimulation modalities including high-frequency (10,000 Hz) stimulation, burst stimulation and dorsal root ganglion stimulation.32-36 These new modalities provide more options for managing pain than historical devices using only one (tonic) mode.
Sedation for interventional pain procedures
Anaesthetic sedation is used in most pain procedures, especially when there are many needle procedures to perform. It is also used if significant allodynia is present. As in usual anaesthetic practice, the patient fasts before the procedure, which is performed in an operating theatre. Some procedures may not be performed if the patient is receiving anticoagulation therapy, unless it is stopped, with some patients needing bridging injections of enoxaparin for up to 18 to 24 hours preoperatively.
Advances in spinal procedural interventions
Current practice for spinal procedural interventions involves imaging guidance, including use of C-arm fluoroscopic devices (image intensifiers), CT and real-time ultrasound imaging. The choice depends on factors such as adequacy of visualisation, which varies depending on the target location, potential radiation exposure with CT, cost to the patient and the overall cost to the healthcare system. The choice, therefore, often also depends on the insurance status of the patient.
Access to procedures and funding considerations
Private health insurance or third-party payers (e.g. workers’ compensation or motor vehicle insurance) enable access to inpatient private pain specialists. Uninsured patients and patients whose procedures will not be paid for by third parties can pay for procedures themselves, or pain specialists can often refer them to interventional radiologists for selected procedures, some of which are partly covered by Medicare. Private out-patient consultations are usually partially covered by Medicare and third-party payers but not by private health insurance. Public government inpatient and outpatient services are usually performed at no direct cost to the patient, and the cost to the government is similar to the private cost.
Take home message
It must be emphasised that procedural pain interventions can provide an additional tool to manage pain symptoms. They must be considered part of the range of socio-psychobiological strategies in pain management. PMT