Clinical use of placebo in pain management

Pain
Modern research has demonstrated multiple specific biological effects following placebo administration in experimental and clinical settings. There is now a challenge to reconceptualise placebo effects as valid psychobiological processes, recognising their presence even if a traditional placebo is not given.
- Placebo effects are part of every healthcare encounter, even if no placebo is given, because the therapeutic ritual is the trigger for placebo mechanisms.
- There are multiple placebo effects, each with unique psychobiological mechanisms.
- There is a shift from deceptive administration of placebo to targeting components of the therapeutic ritual to harness placebo effects (in combination with usual care). Furthermore, initial research augmenting nondeceptive prescription of placebo pills with usual care is promising.
- Understanding placebo effects can improve outcomes for all interventions.
- Nocebo effects can inadvertently lead to increased morbidity and mortality.
- Nocebo effects may play a role when swapping from a branded to a generic medication, so careful exploration of contextual factors may be important in this process.
The word placebo has been used in the medical literature for more than 200 years, with various meanings and connotations ranging from deceptive treatment practices to genuine therapeutic targets in clinical practice.1 Much of the conceptual difficulty with the word placebo has been with its traditional meaning, in that it is an intervention that should be ‘inert’. Although the physical substance (the placebo itself) may be ‘inert’, the neurobiological effects are not, thereby demonstrating a major conceptual problem.
Placebos are not inert; rather placebo administration simulates a treatment ritual that has the potential to trigger a host of endogenous mechanisms (placebo effects) that can relieve symptoms across many conditions. If the placebo is replaced with a specific biological agent (e.g. an opioid analgesic), part of the response to administration of that drug is due to the pharmacology of the drug and the other part is due to the psychosocial context (the so-called placebo component). Therefore, a placebo does not have to be given to achieve a placebo effect.2 These mechanisms are part of routine practice, and are only observed in isolation when a traditional placebo is substituted for a drug, a surgery or any other intervention. On this basis, the multiple elements that encompass the psychosocial context around a patient (including the healthcare practitioner–patient relationship) are potent in either potentiating placebo (positive) or nocebo (negative) effects. The field of placebo research is still in its relative infancy with regard to extrapolating experimental and mechanistic research to the bedside.
Placebo analgesic mechanisms
Research into placebo mechanisms has escalated dramatically in the past 10 years, with much more now known about their specific biochemical and neuroanatomical components across a wide variety of clinical populations. Traditionally, mechanisms (or determinants) have been divided into psychological and neurobiological, which will briefly be explored here in the context of pain.2,3
Placebo analgesic effects have been extensively studied, with assessment of placebo mechanisms in both experimental and clinical pain. From a biological viewpoint, there are several key neuroanatomical changes that occur in the cortex, brainstem and spinal cord after placebo administration that have a significant impact on descending pain modulation systems. The role of opioids has been studied extensively, demonstrating an important and target specific role for endogenous opioid-mediated placebo analgesia.4 More recently, the role of endogenous cannabinoids has been studied, clearly demonstrating at least two discrete endogenous placebo analgesic mechanisms, one that involves opioids and one that involves cannabinoids.4 This is remarkable evidence of multiple placebo analgesic effects.
From the psychological viewpoint, there are several key determinants of the placebo effect.5 Learning processes have been shown to modulate placebo analgesic effects, either through classical conditioning or social learning (whereby witnessing others responsiveness to a placebo enhances one’s own response).6 Expectation of response (benefit) has been the major cognitive determinant, with larger expectations of benefit leading to larger placebo effects. This is enhanced if a conditioning paradigm is used.7 There is now broader exploration into psychological factors, namely those that form the psychosocial context around a patient. For example, a patient choosing to take a placebo enhances the placebo responsiveness,8 as does strategic enhancement of the ‘healthcare practitioner–patient relationship’.9 Augmentation of both verbal and nonverbal cues in the healthcare practitioner–patient relationship resulted in significantly larger placebo effects. Key verbal components included focused questioning of a patient’s understanding of their condition (cause and meaning) and their symptomatology, particularly as it related to lifestyle and function. Furthermore, communication was delivered in a confident and positive manner. Key behavioural elements included:
- presenting in a warm and friendly manner
- active listening
- thoughtful silence.
The complexity of the therapeutic relationship (and its inherent power to trigger what we call placebo effects) has resulted in the need for further research from neurobiological, behavioural and social–psychological viewpoints.
Clinical application
Most placebo and nocebo research to date has been experimental in nature, so therefore there is still a need for more clinically relevant research. There are, however, several contemporary applications of placebos with some scientific support and these are the focus of ongoing research and will be discussed below.
‘Unblinded placebos’ – the nondeceptive administration of a placebo
The primary ethical issue with placebo use is deception and the potential effect this may have on the healthcare practitioner–patient relationship.10 Despite this ethical issue, there are growing data suggesting significant use of placebo in both general and specialist medical care, either of inert placebo or of an ‘active’ medication for incorrect purposes (such as antibiotics for a viral illness).11 Regardless of the content or intention, this is effectively placebo use – that is, providing a therapeutic ritual for its psychobiological effect. Interestingly, results of early tests of so-called nondeceptive or ‘open-label’ placebo use were positive12 and have led to some very interesting recent studies.
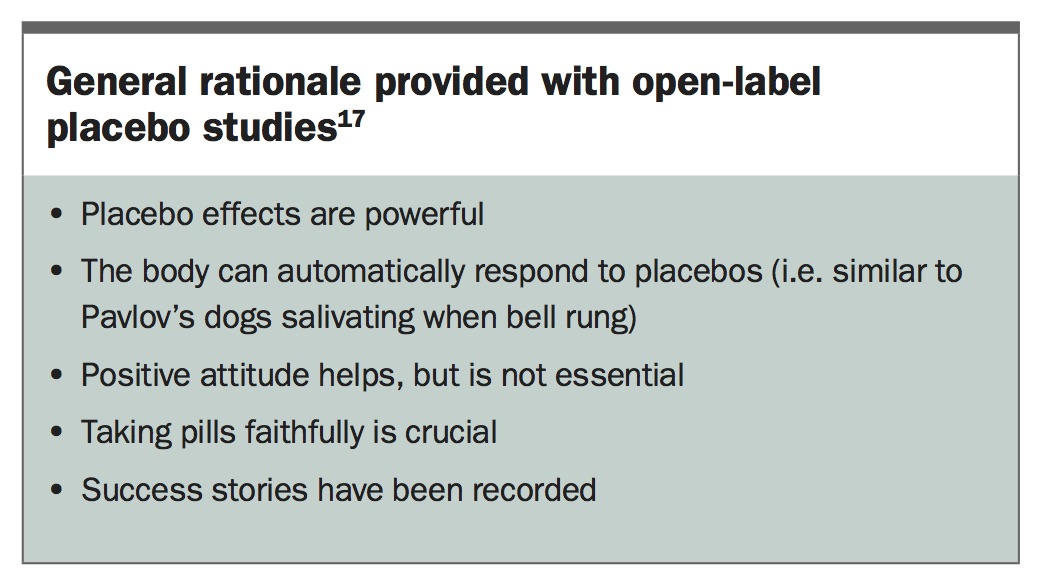
Recent open-label studies have demonstrated statistically signifcant, and in some cases clinically significant (reduction in pain by more than 30%), differences in patients prescribed an open-label placebo without deception, compared with no treatment. To date, these open-label trials have reported benefits for patients with ADHD, irritable bowel syndrome, major depressive disorder, allergic rhinitis and chronic low back pain.13-17 The most recent proof-of-concept study demonstrated that when placebo is added to treatment for chronic low back pain and a plausible explanation is given (Box), there were statistically significant changes in both pain ratings and pain-related disability, compared with treatment as usual.17
{kind=link}
Open-label placebos represent an interesting future treatment avenue for augmenting endogenous placebo mechanisms and have the potential to enhance the efficacy and reduce the side effects of the index drug.
It is emphasised that this is proof-of-concept work at present and is preliminary in its clinical application. Nevertheless, many of the contextual features manipulated in these studies are applicable when prescribing routine medicines and enhancement of such messages may represent a positive application of this research.
Open-hidden paradigm
The most compelling evidence for placebo effects comes from the open-hidden study design, whereby a drug is either:
- administered openly by a physician with normal clinical cues, interactions and context, or
- administration is hidden and occurs through a computer-delivered infusion with no physician in the room. To reduce bias, the same drug and dose were delivered to the patient at random intervals by the computer-controlled infusion. Both the experimenter and patient were not aware of when or what doses of the drug were delivered until after the experiment, thereby removing many of the components of the therapeutic ritual.18
Remarkably, many routinely used analgesics are far less effective when given in the hidden manner with most, if not all, of the placebo mechanisms removed. In fact, morphine is up to 50% less effective when it is given without a therapeutic ritual.19 Similarly, the open-hidden paradigm illustrates the power of drug removal. Open interruption of an infusion resulted in more rapid and significant return of pain than hidden removal, with pharmacological variables controlled. This paradigm underscores the essential principle that the overall outcome of a therapy is the therapy itself and the contextual effects surrounding its administration, which trigger placebo mechanisms.
Nocebo effects
The neurobiological power of words
The experience patients have before, during and after every healthcare interaction unfortunately may not set them up to harness or augment the placebo component of their therapy. In fact, it is possible that the less studied, but equally important, counterpart of the placebo effects, the nocebo effects, can be augmented. Nocebo effects are similarly real biological effects, but their results are negative and attributable to a negative therapeutic context. The classic example is where patients experience side effects in the placebo arm of a controlled trial – in this case it is the negative therapeutic context not the placebo pill that is important. These adverse results can be significant in both number and severity.20
At least three broad elements may play a role. Firstly, negative verbal suggestion or written information given in the informed consent process can lead to modulation in nocebo effects.21 Secondly, expectations shaped by past experience represent an important source of potentially negative information and are therefore a target of the healthcare practitioner–patient intervention. Thirdly, broader environmental factors such as advertising, branding and media coverage can also play considerable roles.22 This underscores the importance of the disclosure process, assessment of patient expectations and past experiences, and broader evaluation of the patient in their particular psychosocial context.
Healthcare communication
Undoubtedly the harnessing of placebo effects is essential for treatment optimisation, particularly for symptomatic relief rather than disease cure.23 However, nocebo effects may have the potential to elicit a more profound effect on morbidity and mortality. For example, a recent two-year prospective study in women with hormone receptor-positive breast cancer who were due to undertake adjunct endocrine treatment showed that women with pretreatment negative expectations about side effects were almost twice as likely to report side effects than those who had minimal or no negative prior expectations.24 Of particular importance, the pretreatment expectations of treatment side effects predicted both health-related quality of life and adherence to treatment. This was a small effect but very relevant as adherence to adjunct endocrine treatment predicts survival rates and is therefore a potentially important link to morbidity and even mortality.
Although this is an extreme example of potential consequences or pretreatment expectations, it is important because this is a potentially modifiable factor that all clinicians can influence. One way to achieve this might be through reframing of the information.21 This was demonstrated in a study of the administration of epidural analgesia during labour.25 In one group the information was negatively framed and they were told ‘you are going to feel a big bee sting; this is the worst part of the procedure’. A second group had the information framed positively and were told ‘we are going to give you a local anaesthetic that will numb the area and you will be comfortable during the procedure’. The group receiving the more positively framed information reported significantly less pain.25 This is a clear demonstration of the importance of the way in which information is delivered and its potential effect for iatrogenesis, or at least suboptimal use of endogenous placebo effects. It has been suggested that efforts should be made during all interactions, especially around informed consent, to avoid instilling negative expectations in others.21 One needs to constantly be aware of how communication influences both positive and negative outcomes.
Medication branding
Logically, it would be presumed that medications with the same active ingredient would work equally as well, despite the label. However, not all medications are perceived as being created equal. Interesting experimental work on individuals with headache pain demonstrated greater analgesic effect for a branded medication compared with a generic medication.26 To resolve this issue, a recent study provided education which improved participants’ understanding and perceptions about the generic medications.27 However, an important finding for prescribers and pharmacists to consider is that despite these improved perceptions about generic medications, it did not lead to better patient outcomes. Instead, the opposite occurred with the educated group reporting a less beneficial effect and more side effects with the generic medication, even though the active ingredient was identical. This response may in part be determined by an individual’s choice in switching medication, because their placebo mechanisms may be different depending on factors such as trust in the brand or the size, shape or taste of the pill, to name a few possibilities.28,29 This is clearly an important aspect of routine care that requires further research.
Future directions
The most important step in the application of the rapidly growing research on placebo and nocebo effects is the conceptual one. As has been discussed, the many patient and contextual factors that initiate placebo mechanisms also engage these mechanisms when routine analgesic therapy is given. This underscores the notion that you do not have to give a placebo to trigger a placebo analgesic effect. Similarly, negative context (nocebo mechanisms) can be elicited during routine therapy, making this therapy less effective.
The healthcare encounter is the centrepiece of the operation of placebo and nocebo effects. It is the rich psychosocial context surrounding the assessment, diagnosis and management of pain. There are many factors involved in this complex interaction, and these are currently the subject of ongoing research. Nevertheless, several important implications have been discussed here. Firstly, on the back of open-label placebo trials, the possibility that targeted education empowers patients to understand that drug therapy works both through extrinsic and intrinsic mechanisms (the placebo mechanisms) can be considered. Some of the messages in the open-label trials might be useful in routine care. Secondly, the outcomes of most therapies are partly due to the index therapy and the contextual component. Conscious appreciation of this in routine care, including efforts to augment the healthcare practitioner–patient relationship may be particularly useful in improving outcomes.9 Finally, there is a body of research around the power of words, and cautious discussion and disclosure about treatment effects and side effects can potentially minimise nocebo effects to improve treatment efficacy. Also, careful assessment of patients’ expectations surrounding branded treatments may allow for targeted prescription or intervention.
Houston (1938) wrote of ‘the doctor himself as a therapeutic agent’.30 This is applicable to all healthcare providers and its value has only been augmented some 80 years later with the support of a growing body of mechanistic and clinical literature. PMT