Managing pain in patients with rheumatoid arthritis

Rheumatoid arthritis
Pain
Patients with rheumatoid arthritis who are responding to disease-modifying drug therapy but continue to complain of pain – in joints and elsewhere – present a management challenge. Although biomedical factors may play the major role in the pain experienced by such patients, consideration of the psychological and social dimensions is essential. A sociopsychobiomedical framework is useful for patient assessment and for identifying other, nondrug, therapeutic pathways.
- Perhaps every second patient with rheumatoid arthritis will experience ongoing pain and disability despite optimal control of inflammation.
- The sociopsychobiomedical framework for chronic pain is not only useful for assessing such patients but also provides a template for identifying other, nondrug, therapeutic pathways.
- Biomedical factors other than inflammation need to be considered, including the new concept of nociplastic pain.
- Symptom control is important, as an adjunct to nondrug treatment approaches. Australian prescribers have access to a variety of medicines that should be used judiciously.
Rheumatoid arthritis (RA) is the most common of the chronic autoimmune (describing aetiology) inflammatory (describing pathogenesis) diseases affecting joints.1,2 Being inflammatory and polyarticular by definition, it may also affect extra-articular tissues and be associated with systemic illness. Untreated, it will cause damage to articular cartilage and bone, leading to significant disability. It follows that early diagnosis and vigorous treatment to control inflammation and thereby to prevent joint damage are of paramount importance.
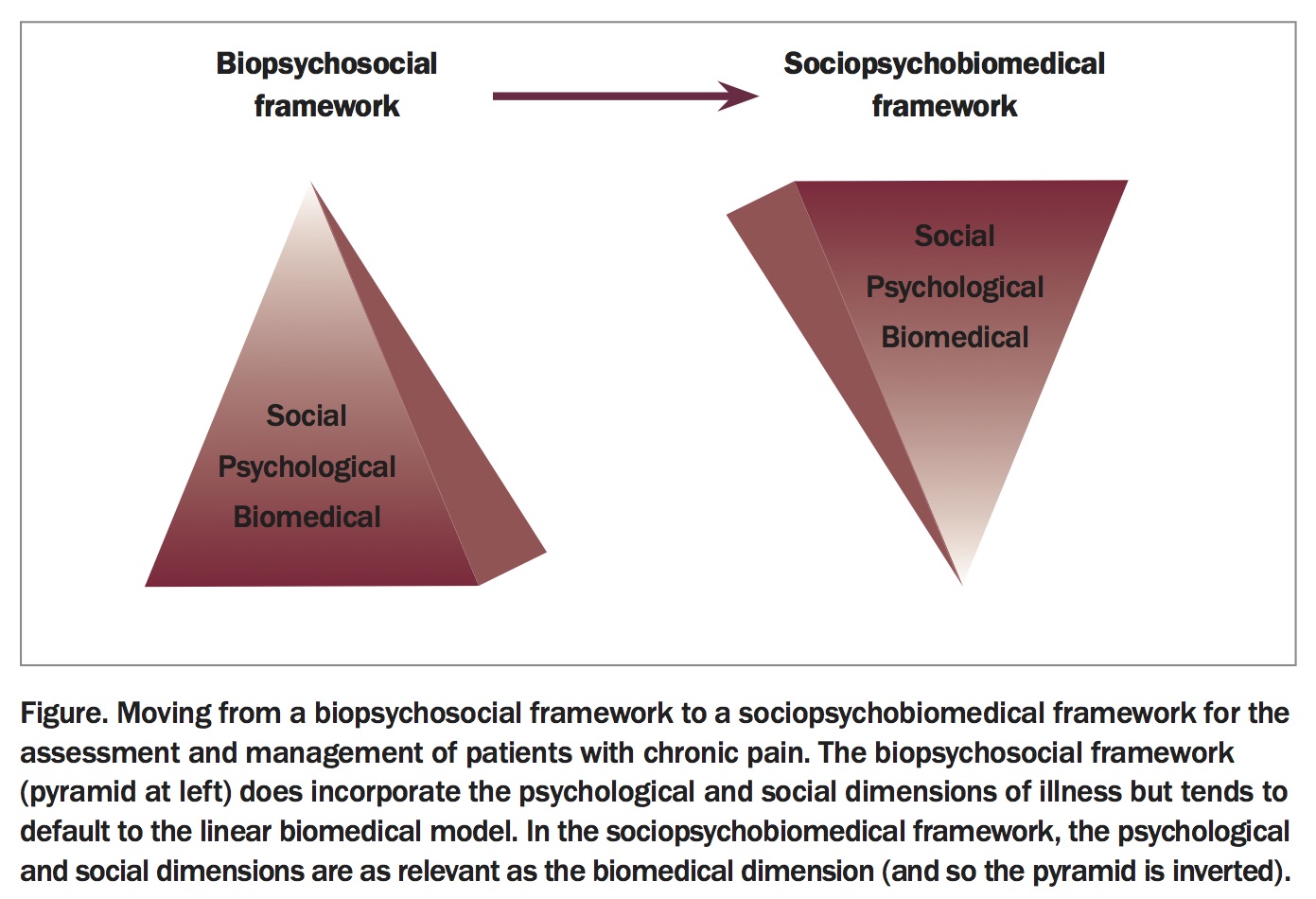
As its name implies, RA is conceptualised mainly in a biomedical model: a known disease process that affects the body via well described biological mechanisms, justifying a therapeutic focus on that dimension. But RA is not so simple, as it is known to be associated with environmental factors such as low socioeconomic status, low level of education and smoking, to name but three.2 Furthermore, the effects on the whole person of having a chronic disease that is painful and tiring and interferes with activity, vocational and recreational, tend to be ignored in therapeutic discussion. This has been partly addressed in chronic illnesses through the prism of the biopsychosocial framework that identifies contributions to pain, disability and suffering in the ‘bio-’ dimension (what is happening to the person’s body), the ‘-psycho-’ dimension (what is happening to the person), and the ‘-social’ dimension (what is happening in the person’s world). However, it has been well recognised that, especially in view of the remarkable advances in biomedicine, this biopsychosocial framework tends to default to the linear biomedical model.3
Despite the logic of treating inflammation in RA, it must be acknowledged not only that not all patients respond optimally but also that pain and disability are not linearly related to what is happening in their joints. From the perspective of the discipline of pain medicine, the recognition that the psychological and social dimensions are just as if not more relevant than the biomedical in chronic pain conditions has led to the inversion of the biopsychosocial model into a sociopsycho biomedical framework for patient assessment and management (Figure).4
{kind=link}
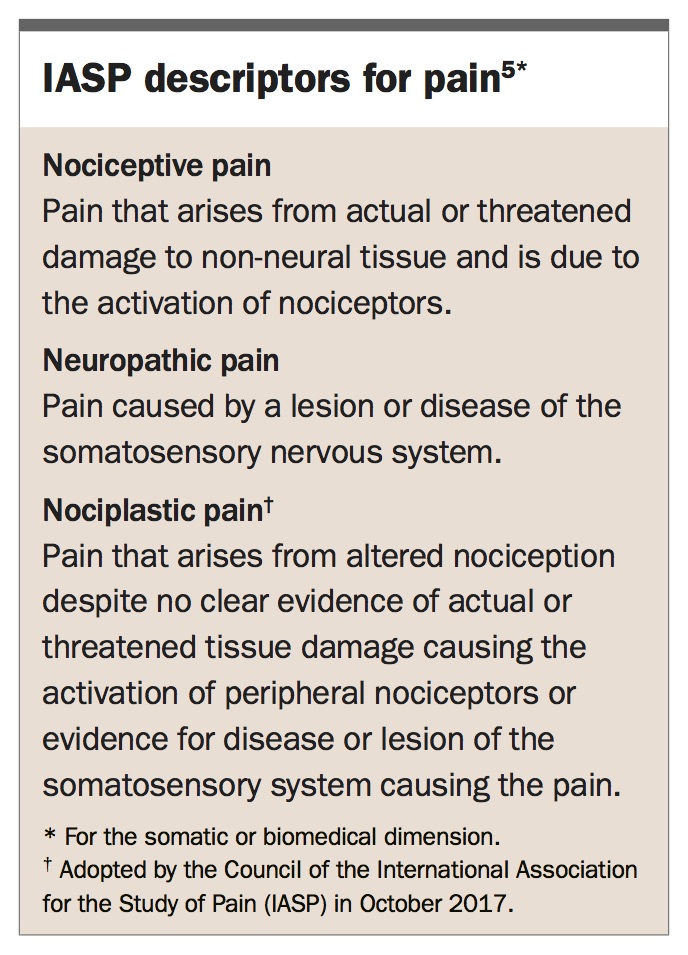
Starting at the bottom of this inverted pyramid shown in the Figure, this article will provide a framework for managing pain in patients with rheumatoid arthritis. Current descriptors for pain are given in the Box.5
{kind=link}
The biomedical dimension
Nociceptive pain
Inflammation, the primary pathogenetic mechanism in RA, is expressed typically as pain. This is an example of nociceptive pain, that is, pain due to activation of nociceptors in response to actual or threatened tissue damage.5 It comes as no surprise that proinflammatory cytokines are pro-nociceptive and that anti-inflammatory cytokines are anti-nociceptive. Indeed the process of inflammation can be seen as characterised by cytokine-induced activation of nociceptors (contributing to pain), sensitisation of peripheral nociceptors (contributing to tenderness [allodynia]) and local changes in tissue permeability (contributing to swelling). All the anti-inflammatory drugs (steroidal and nonsteroidal), and conventional synthetic, targeted synthetic and biological disease modifying agents are directed towards this mechanism. The current state of the science in this respect is well summarised in reference 2 and will not be discussed here.
Another phenomenon that must be considered at this nociceptive level is the pain of joint damage and the pain that comes from altered use of other parts of the body as a result of inflammation and/or damage to a joint. Consider, for example, a patient whose knee inflammation has come under good control but who has some loss of femorotibial cartilage with a mild valgus deformity on weight-bearing. This patient may complain of pain not only in the knee but also related to the ipsilateral ankle and foot or the contralateral hip joint or the lumbar spine, even though those joints haven not been affected by the inflammatory process. It is probable that this latter pain is related to gait abnormality, to which relative muscle weakness might contribute. The mechanisms of mechanical activation of nociceptors remain poorly understood: what is well recognised is that NSAIDs are only poorly effective in noninflammatory joint pain.
The therapeutic implications here include identifying and correcting altered gait, actively through targeted re-education and strengthening of muscles, and passively through the use of footwear, orthotics or walking aids. In the case of affected upper limb joints, modification of usage patterns and the use of splints or labour-saving devices are variations on this approach.
Neuropathic pain
Neuropathic pain, which is commonly over-identified, is in fact not a diagnosis but the descriptive term for pain caused by disease or damage of the somatosensory nervous system.5 This descriptor can be applied only when there is a demonstrable lesion or a disease that satisfies established neurological diagnostic criteria. In other words, adjectives (such as burning, pricking, stinging) or even features such as touch-evoked pain (allodynia) on their own do not justify that descriptor: there must be signs of neuropathy.
In the context of RA, peripheral neuropathy may be due to compression – of the median nerve in the carpal tunnel, of the ulnar nerve in the cubital tunnel, of the posterior tibial nerve in the tarsal tunnel, or of digital nerves secondary to subluxed metatarsophalangeal joints – or, less commonly, to vasculitis. In the case of severe affection of the cervical spine by the rheumatoid process, cervical radiculopathy and/or cervical myelopathy may occur. All these examples, which may be sources of pain, require clinical demonstration of axonal dysfunction, such as motor weakness in a peripheral nerve or myotomal distribution and/or reduced cutaneous sensation in a peripheral nerve or dermatomal distribution, possibly associated with reduced deep tendon reflexes in the case of radiculopathy.
Therapeutically, compression neuropathy is managed best through chemical control of (teno-)synovitis, including perineural corticosteroid injection, splinting or often surgery. Axonal sensitivity, whether due to compression or vasculitis, may be rationally addressed with agents such as gabapentin or pregabalin but the responses are poor: the number needed to treat for gabapentin is 6.3 (95% confidence interval [CI], 5.0–8.3) and for pregabalin is 7.7 (95% CI, 6.5–9.4).6
Nociplastic pain
Prior to the redefinition of neuropathic pain in 2011 (see section above), pain that was not nociceptive was commonly deemed by default to be neuropathic, as the earlier definition for neuropathic pain included ‘dysfunction of the nervous system’.7 However, the redefinition specifically excluded dysfunction, which left a large group of patients who had evidence of altered nociceptive function without a valid pathophysiological descriptor for their pain. That void has now been filled, with the recent adoption of the term nociplastic to describe pain states characterised by clinical and psychophysical findings that suggest altered nociceptive function, such as static and dynamic mechanical allodynia elicited in normal tissues.8 The term nociplastic (from nociceptive plasticity) was developed specifically to imply a central mechanism, namely plasticity – including modulation – of nociceptive pathways in the central nervous system. This term has been preferred to the misnomer, central pain.
There is much evidence to suspect that altered nociceptive function plays a role in RA, including pain and increased sensitivity to mechanical stimuli – touch, pressure, movement – in a distribution more widespread than joints alone. This is often referred to as concurrent fibromyalgia.9 The mechanism underpinning these phenomena is considered to be central sensitisation of nociception, itself a response to sustained nociceptive input such as would be expected in a chronic inflammatory condition such as RA.
These three pain descriptors might coexist in the one patient at the one time, especially nociceptive (from peripheral joint inflammation or biomechanical problems) and nociplastic (from changed central nociceptive function, such as central sensitisation). An important principle is that damaged joints, which are often sensitive in a neurophysiological (nociceptive) sense, need to be protected from ‘overuse’, which in many instances is the patient trying to use them in the same way as before they were affected by arthritis.
Given the recent evolution of these terms and concepts, the literature has not yet addressed specific treatment approaches to nociplastic pain, although the pharmacological tools available are the same as those used in (true) neuropathic pain – namely tricyclic antidepressants, serotonin–noradrenaline reuptake inhibitors and gabapentinoids. There may be role for a trial of these medications in some patients.10
The psychological and social dimensions
Discordance between clinical and laboratory evidence of inflammation and pain, disability and fatigue in patients with RA has long been documented. In a recent cohort study of patients with established RA, just under half reported moderate to high levels of pain and fatigue. Most of these patients had minimal inflammation but high scores in instruments that measure mood (depression and anxiety), sleep problems and pain catastrophising.11 An earlier longitudinal study of more than 500 patients with RA over eight years looked at factors such as perceptions about adequacy of social support, self-assessed ability to cope with RA and satisfaction with health and function, and found that depressive symptoms and function over time were more closely linked to these psychosocial risk factors than to disease factors.12 Earlier work still found outcomes in RA to be related to education and socioeconomic status rather than necessarily to biomedical indices.13
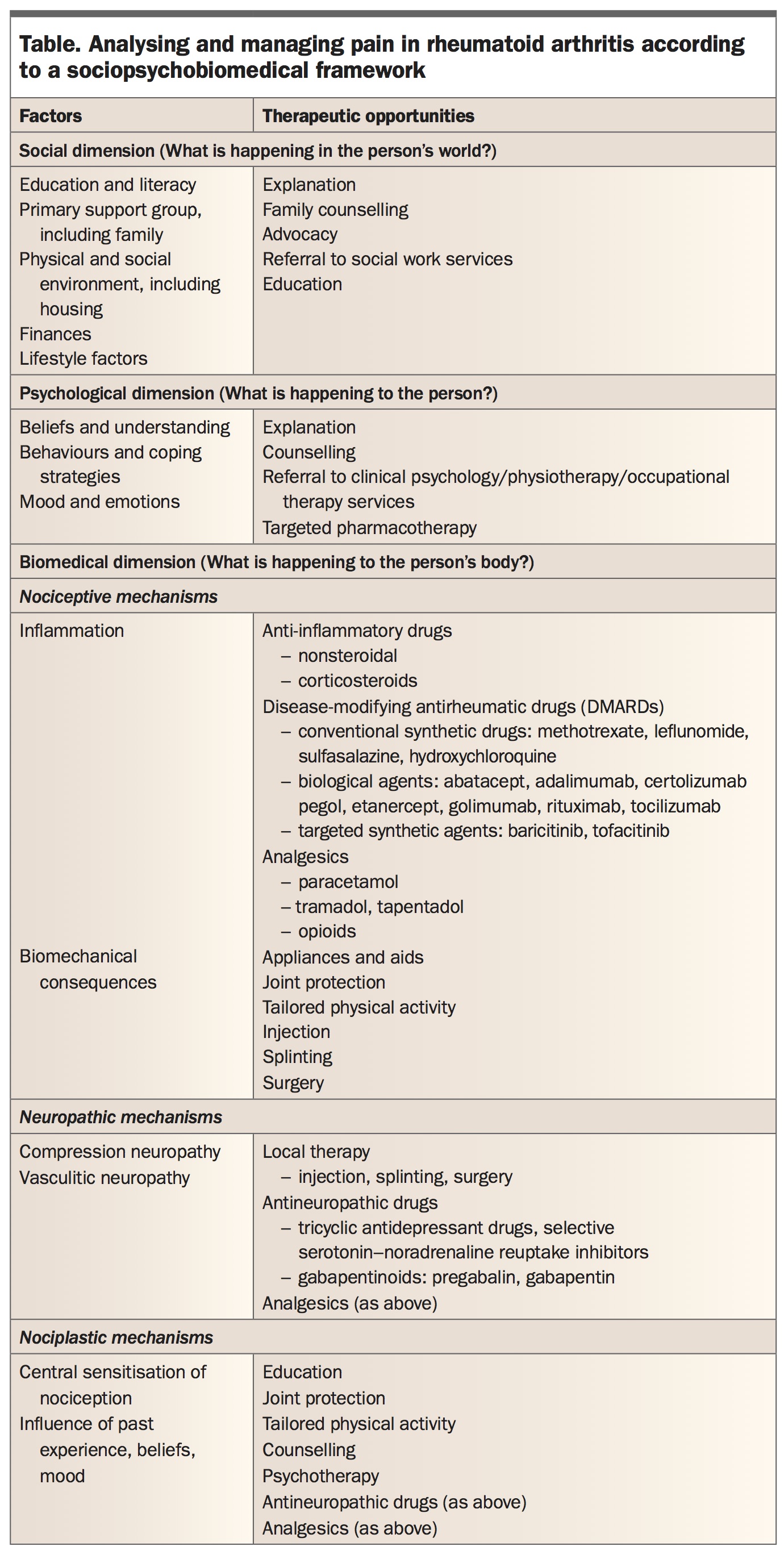
These studies and others highlight that what is happening to the person (the psychological dimension) and what is happening in the person’s world (the social dimension) are important determinants of outcome in a chronic disease such as RA, manifest most commonly as pain (which may also be a code for multifactorial distress) and disability (which varies according to context). Other important factors here are comorbidity and the effects of polypharmacy. In effect the experience of chronic pain in RA is not biologically different from that in other instances of chronic noncancer pain, with the possible exception that validation of the patient’s predicament is more easily forthcoming due to its visibility and plausibility.3,4 (See Table).
{kind=link}
Analgesic strategy in RA
Although identifying and addressing factors in the social and psychological dimensions is essential when analysing distress in a patient with RA, those factors may not be amenable to medical intervention. Thus, especially in primary care, the need for symptom control over and above disease control often defaults to the use of analgesic medications.
In the BEACH study of chronic (noncancer) pain conducted in primary care in Australia and published in 2013,14 86% of the 1074 respondents in whom pain management was reported took at least one analgesic medication. Of these, 43% (95% CI, 41–45) took paracetamol, 21% (95% CI, 20–22) took NSAIDs and 34% (95% CI, 31–37) took opioids. Of the last of these, combinations of codeine 30mg were the most frequently used. Notably, in this study 38% (95% CI, 35–41) reported using nondrug management techniques in addition to or instead of medication.14
The use of paracetamol and NSAIDs in RA is uncontroversial, although not necessarily effective. With respect to opioid analgesic use in RA, a Cochrane review published in 2011 concluded that the limited evidence for the effectiveness of weak oral opioids in some patients was overshadowed by adverse effects, whereas no conclusions could be drawn about the use of strong opioids or the prolonged use of opioids.15
Recently there has been a plethora of publications regarding the use of opioid analgesics in chronic noncancer pain, with the triple themes of increasing prescription, insufficient evidence of long-term effectiveness, and harms (adverse effects, addiction and overdose) outweighing benefits.16,17 The drivers for this have been well identified, especially injudicious prescription, despite the ready availability of guidance.18,19
Given that opioids remain the most effective analgesic agents overall, does this mean that there is no role for them, in the current climate, for persistent pain associated with RA? The sociopsychobiomedical framework for assessment of all types of chronic non-cancer pain is also a template for management that emphasises a multidisciplinary approach in which drugs play an adjuvant – not a primary – role. The judicious prescriber will recognise that a trial of opioid for pain associated with RA may be reasonable, especially when adjuvant agents such as tricyclic or serotonin–noradrenaline reuptake inhibitor gabapentinoids or other analgesics such as tramadol or tapentadol have been associated with inefficacy or intolerance.20
A summary of management strategies for treating pain in patients with RA, arranged according to relevant factors in an individual patient’s social, psychological and biomedical dimensions, is presented in the Table.
Conclusion
Although biomedical (disease) factors may play the major role in the pain experienced by patients with RA, that may not be the whole story in many cases. A sociopsychobiomedical framework for assessing those who are not ‘doing well’ may identify other, mainly non-drug, therapeutic pathways. However, symptom control remains paramount, in which respect the Australian prescriber has access to a variety of different medicines that might be used on a trial basis, including opioids according to current guidance. PMT