Managing neuropathic pain after surgery
Pain
Neurological diseases
Once persistent neuropathic pain after surgery is established, treatment can be difficult but should be individualised, multimodal and, if necessary, multidisciplinary. The ultimate goal is to restore function and quality of life rather than exclusively target pain scores.
- Surgery is an increasingly common cause of persistent neuropathic pain. About 20 to 50% of patients experience persistent pain after surgery, with severe pain occurring in 2 to 10%.
- Prevention by avoidance of unnecessary surgery is a key strategy while more research into risk stratification and pharmacological preventive strategies is being pursued.
- The treatment of neuropathic persistent postsurgical pain (PPSP) should be individualised, multimodal and, where necessary, multidisciplinary. Patients with PPSP that is severe and/or causes high levels of disability or distress should be referred to a pain management unit.
- PPSP that is neuropathic should be treated according to current guidelines; however, there is limited evidence to help guide prescribers. Opioid medications should be used with caution after the immediate perioperative period.
More than 230 million people undergo surgery each year worldwide,1 and all of these operations have the potential to cause persistent postsurgical pain (PPSP). Reported figures vary, but a reasonable estimate is that 20 to 50% of patients experience PPSP, with severe pain occurring in 2 to 10%.2 The neuropathic component of this pain is likely to be substantial and under-recognised and therefore undertreated.
PPSP is defined as pain that:
- lasts at least three months after surgery
- is not present before surgery or has different characteristics or increased intensity from preoperative pain
- is localised to the surgical site or a referred area
- occurs when no other causes of the pain (e.g. infection, cancer recurrence) are found.3
The economic burden of PPSP has been estimated at US$41,000 per patient per year.4 This is the result of increased healthcare utilisation and the opportunity cost of poor recovery in otherwise healthy adults. Cancer survivors in particular appear to be at increased risk of neuropathic PPSP. Increasing survival rates combined with high levels of psychosocial distress lead to a significant burden on these patients, their families and the community in general.
The International Association for the Study of Pain (IASP) had a ‘Global Year Against Pain After Surgery’ in 2017. Information and resources for patient education are available online for free (www.iasp-pain.org/GlobalYear/AfterSurgery).
Pathophysiology of PPSP
The damage, stretching and inflammation of tissue that occurs during surgery leads to activation of pain-specific nerve fibres (C fibres). This information is then carried to the central nervous system and on to higher centres via the contralateral spinothalamic and spinoreticular pathways to cortical and subcortical centres in the brain where pain is further processed and, ultimately, consciously experienced.5
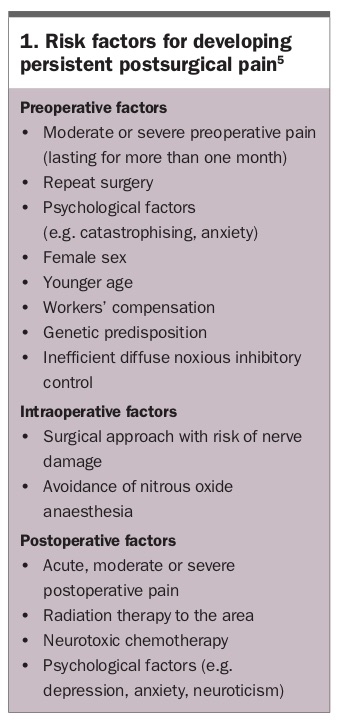
Several changes happen within the central and peripheral nervous system during this acute activation. In most patients these changes are reversible; however, they may become permanent, leading to potential PPSP. It is becoming increasingly evident that tissue injury following surgery leads to changes in the functioning of pain pathways that are unique to incisional injury.1 Incisional pain appears to have greater potential to become centrally sensitised than other types of pain injuries such as fractures or contusions. Active research is underway to determine which aspects of multimodal analgesia may be more helpful given the unique mechanisms of incisional pain. Known contributors of risk for PPSP are listed in Box 1.5
{kind=link}
The transition of acute postoperative pathological persistent pain is complex and only partially understood.6 There is likely a complex interaction between the patient’s environment (biological, psychological and social factors) and a susceptible genetic profile which is involved in perpetuating the pain.7
Damage to nerves, particularly major ones, appears to be a common cause of PPSP. Patients who undergo surgeries in which nerves are commonly damaged (e.g. amputations, thoracotomies, cardiac surgery and breast surgery) have the highest rates of PPSP.8 However, not all patients with damaged nerves go on to develop PPSP and pain can occur in the absence of nerve sectioning.9 To illustrate the degree of uncertainty around the role of nerve injury in PPSP, the most recent international consensus guidelines in inguinal hernia surgery recommend division of the ilioinguinal nerve if encountered during surgery as this seems to reduce the incidence of neuropathic pain afterwards.10 This is contrary to the generally accepted view that deliberate nerve transection in surgery increases the risk of PPSP.
Some of the intraoperative modifiable factors include the type, length of time and technique of surgery. There is a lower incidence of PPSP in laparoscopic as opposed to open surgeries.11
Potential for prevention of neuropathic PPSP
Once neuropathic PPSP is established, treatment can be difficult. Unsurprisingly, there is increasing interest in techniques that may prevent neuropathic PPSP. The most obvious and effective way to pragmatically prevent postsurgical pain is to avoid unnecessary operations. Procedures with a poor evidence base or for which there are nonsurgical alternatives – for example, arthroscopies for osteoarthritic knee pain – should be avoided altogether. Operations such as lumbar decompression or fusion should only be performed in clinical situations for which the evidence is clearly supportive. Warning patients before surgery as part of the process of informed consent should be part of any preoperative work up with the current level of knowledge regarding risk of PPSP.
Anaesthetic techniques and postsurgical acute pain management likely play a role in the prevention of PPSP. The management of acute postsurgical pain has traditionally been largely opioid based. There is now an increased emphasis on multimodal management. Poorly controlled acute pain has been linked to the development of PPSP, and improved acute pain control may in some cases prevent PPSP.
Regional techniques may be beneficial for some surgeries. Notably, epidural analgesia may prevent PPSP after thoracotomy and paravertebral blocks may prevent PPSP in women undergoing breast cancer surgery.12 Perioperative ketamine has produced positive but inconsistent results thus far;13 however, currently a major multicentre Australian trial known as Reduction of Chronic Post-surgical Pain with Ketamine trial (ROCKet) is attempting to determine its perioperative usefulness in preventing PPSP (https://medicine.unimelb.edu.au/research-groups/medicine-and-radiology-research/appmu/appmu/the-rocket-study).
In the acute perioperative setting, multimodal pharmacological strategies, psychological strategies, modified surgical techniques, procedure-specific postoperative pain management and enhanced postoperative recovery programs are all used to prevent persistent acute postoperative pain.5,14
The concept of a transitional pain service to support patients with complex acute pain after discharge for up to three months is gathering support both in Australia and overseas. The business case for such clinics is robust, given the lifetime costs of treating patients with neuropathic PPSP,4 but the development of such innovative services will rely on the vision of tertiary hospitals.
Considering a diagnosis of neuropathic PPSP
If a patient presents to their GP with what appears to be excessive pain following an operation, a multifaceted assessment is required. History should include an assessment of the risks for PPSP and postoperative factors that may have contributed to the ongoing pain, such as overuse of the injured area or failure to adhere to recommended precautions. Symptoms of fever, malaise and reports of swelling and rubor should not be missed. Examination should assess wound integrity and careful delineation of the territory of the pain. If needed, investigations should be used to exclude the potential of concerning or reversible causes such as tumour recurrence, infection or nonunion of bone. An opinion should be sought from the treating surgeon as to whether the ongoing reports of pain fall within or outside the expected trajectory of healing for the procedure concerned.
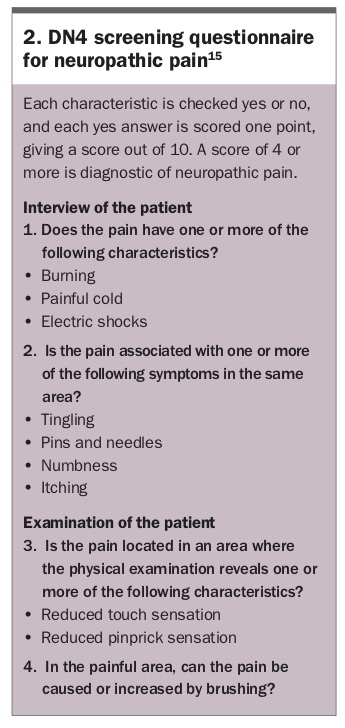
Questionnaires such as the Douleur Neuropathique 4 (DN4) can be helpful in screening patients in whom neuropathic pain is considered (Box 2).15 The sensitivity and specificity of the DN4 were estimated at 90% and 60%, respectively, for detecting chronic neuropathic pain at six months of follow up in patients who had undergone breast cancer surgery.16 Once the diagnosis of PPSP has been suspected by exclusion of an obvious treatable pathological cause, then additional features of the pain complaint should be elucidated including screening for neuropathic features. Diagnosis is based on symptoms suggestive of neuropathic pain along with positive and negative signs on examination, and should follow the Flowchart.17
{kind=link}
Does the patient have complex regional pain syndrome?
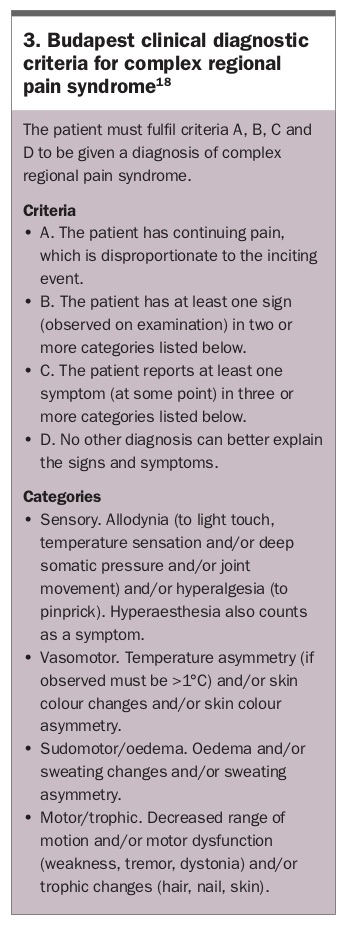
Complex regional pain syndrome (CRPS) is a quasi-neuropathic pain disorder that is incompletely understood. The pain of CRPS is typically regional, affecting the distal part of a limb, and has a neuropathic quality to it. Other signs and symptoms may reflect dysfunctional neurological phenomena in the areas of motor control, sweating, thermoregulation and trophic changes to skin, hair and nails. CRPS is uncommon but the diagnosis is important to make. The Budapest criteria are the clinical gold standard for diagnosing CRPS (Box 3).18
{kind=link}
Strong suspicion of CRPS should trigger urgent referral of the patient to the most accessible pain management unit, as treatment is specialised and early diagnosis is believed to improve long-term prognosis for this highly distressing and disabling condition.
Treatment
The management of neuropathic PPSP is poorly researched and guidance is based on largely anecdotal evidence and expert consensus. The ultimate goal of treatment is to restore function and quality of life rather than exclusively target pain scores. If the pain meets criteria for diagnosis of neuropathic pain then it is appropriate that the IASP neuropathic pain guidelines are followed.19 The National Prescribing Service (NPS) has also published comprehensive diagnostic and treatment recommendations for neuropathic pain in collaboration with the Faculty of Pain Medicine (www.nps.org.au/medical-info/clinical-topics/news/neuropathic-pain-diagnosis-and-treatment-today).17 These guidelines provide the best available consensus for pharmacological management of neuropathic pain, and are based on the consensus recommendations of the IASP.19 They recommend four first-line medicines for the treatment of neuropathic pain, which are amitriptyline, duloxetine, gabapentin and pregabalin. Other medicines recommended as second- or third-line options include tramadol, lignocaine, capsaicin and botulinum toxin A.
Strong opioid medications are regarded as third-line therapy for patients with neuropathic pain. As in other types of chronic nonmalignant pain, the appropriate role for these drugs is not determined on the basis of current evidence. The initial modest efficacy declines over time in most patients. As recommended in the Faculty of Pain Medicine Choosing Wisely advice (www.choosingwisely.org.au/recommendations/fpm), strong opioids should not be used as monotherapy and should be subject to ongoing demonstration of functional benefit, periodic attempts at dose reduction and close monitoring for the known harms of prolonged use at moderate or high dose.
For patients with significant disability or severe pain, a referral to a multidisciplinary pain clinic is recommended. These clinics can give guidance for medication use and other pain interventions, as well as treat psychological and physical comorbidities. Advanced pain therapies for neuropathic pain such as percutaneous and implantable electrical stimulation, ketamine infusions, botulinum toxin and radiofrequency modalities may be offered if appropriate once less invasive treatments have been exhausted. These treatments should only be provided in specialist centres with the ability to manage possible complications and situate the procedures within the wider program of rehabilitation efforts.
Conclusion
Surgery will continue to be a common cause of neuropathic pain in Australia and is likely to increase as the complexity of surgery increases and perioperative mortality continues to decrease. An awareness of the risk of neuropathic PPSP for a specific patient undergoing a particular procedure should ideally be part of the perioperative assessment and consent process.
Significant research into prevention for high-risk operations is currently being undertaken, and this is largely centred on surgical and anaesthetic techniques. Pragmatically, encouraging patients to shun low-value surgery is probably the most effective prevention strategy at present.
Recognition of neuropathic pain can be aided by use of recognised screening tools such as DN4, and CRPS should be suspected in any patient who has had limb surgery and has developed pain out of proportion to the original surgical insult. Patients meeting the Budapest criteria should be urgently referred to a pain management unit for assessment if no clear anatomical cause can be determined by the treating surgeon and GP.
Once neuropathic PPSP is established, treatment can be difficult but does not depart from the standard approach to any neuropathic pain. Patients who are very disabled or who have severe pain should be referred to a tertiary pain clinic if there is inadequate improvement with use of first- and second-line pharmacological therapy according to the NPS/IASP guidelines. Opioids should be used with appropriate caution and monitoring, as third-line therapy, if their use demonstrates ongoing functional benefit and the side effects are acceptable. PMT