Pain in adolescence: a time of vulnerability and opportunity

Pain
Adolescent health
Pain in adolescence and youth can interrupt learning, social outcomes and work roles with life-long effects. GPs can help young people to reduce their pain and disability, and can co-ordinate care if allied health or specialist advice is needed. A focused approach in adolescence may restore wellbeing and prevent persisting pain in adulthood.
- In Australia, 14% of people with chronic pain are young people.
- Headache, abdominal pain and musculoskeletal pain are common in adolescents. Pain associated with surgical or traumatic nerve injuries may be under-recognised.
- A tailored explanation of the diagnosis and answers to a young person’s questions are foundations for engagement in treatment.
- Analgesics may help some young people, but should not be stand-alone treatment. Consent, timeframe, goals, review of adverse effects and deprescribing should all be part of a medication plan.
- Face-to-face school attendance is vital and even therapeutic for school-age adolescents with pain.
Picture credit: Ademortuus/iStockphoto.com Model used for illustrative purposes only.
Adolescence is a period of transition between childhood and adulthood, associated with major biological and social changes. It is a time of knowledge and skill acquisition, and exploration of interests and relationships. Adolescents or young people aged 12 to 24 years comprise 18% of the Australian population.
Although 93% of adolescents in Australia rate their health as good to excellent, there are growing concerns for their future health.1 Only 44% meet guidelines for physical activity, 5% meet nutritional guidelines, 35% are overweight or obese, 19% have used illicit drugs in the past 12 months and 13% have a substance abuse disorder.1 Furthermore, 38% of Australian youth are highly concerned about stress,2 and suicide is the second leading cause of death.1 Pain cannot be managed in isolation from these other determinants of adolescent health and wellbeing.
Pain in adolescence
Contrary to widely-held belief, pain in adolescents is common.3,4 The most prevalent conditions are headache (54%), abdominal pain (50%) and back pain (37%), and these pains frequently coexist.4 Girls have a higher prevalence of pain than boys and prevalence increases with age.4
Chronic pain during adolescence and youth is a significant public health concern.5 In Australia, 5 to 19% of 15- to 24-year-olds experience chronic pain that interferes with daily activity.6-8 In the short term, this is associated with seeking professional help, using medications, school absenteeism, reduced activity levels, reduced quality of life and social isolation. In the longer term, work, health and social outcomes may be affected throughout adulthood. Intervening early is a good investment.
Understanding and managing pain in adolescence is best achieved in a family context. Not surprisingly, 99% of 12- to 17-year-olds live with a parent, as do 57% of 18- to 24-year-olds.1 Pain during adolescence impacts the whole family’s resources – time, work, finances and emotions. Conversely, a young person’s ability to cope with pain may be influenced by their parents’ chronic pain experiences and health behaviours. A family GP is well positioned to appreciate these complex interactions and match management to them.
Clinical approach by the GP
A trusting relationship with adolescents and their carers is key to engagement and success. Adolescents with chronic conditions or persisting pain want:9-11
- to be listened to
- to be believed
- to have their hope for a full recovery acknowledged
- inclusion of and respect for their family as per their wishes
- clinicians to be thoroughly honest and caring
- clinicians to have expertise in managing their chronic illness
- good communication between healthcare providers.
The adolescent should tell their own story whenever possible. If a supporting adult is present, the adolescent should be addressed from the start, asking them to introduce the adult. When the adolescent is ready, usually at about 14 years of age, they should be seen alone for at least some part of each appointment. This helps the young person grow self-report skills and allows confidential disclosure of social safety, risks and stressors.
History
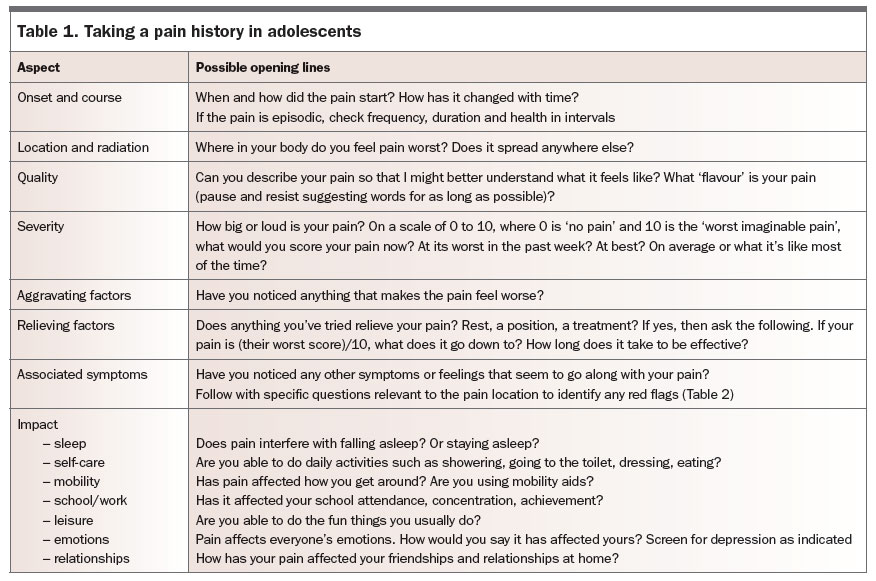
If a GP knows the adolescent and their family well, a focused pain history will often suffice (Table 1). However, if the adolescent’s background is incompletely known, it is vital to gather general health, family and psychosocial information to understand the context in which the pain is experienced, and who might support the young person in managing it.
{kind=link}
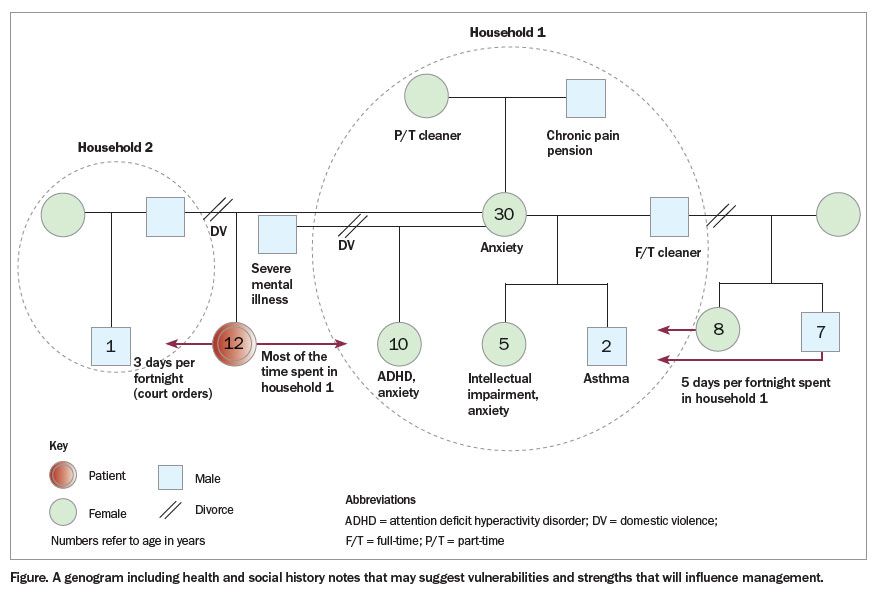
A genogram or family tree can help paint a picture of the adolescent’s family history and home environment (Figure). All people who live in the household should initially be enquired about, and then the extended family supports, any missing partners, length of separations and any regular contact or shared parenting. Work and other roles should be noted, and also the physical and mental health of each household member, noting any potential familial conditions. Finally, how the adolescent gets on with household members, including siblings, should be asked about. Although software exists for genograms, it does not yet interface with GP systems, so time and paper are required.
{kind=link}
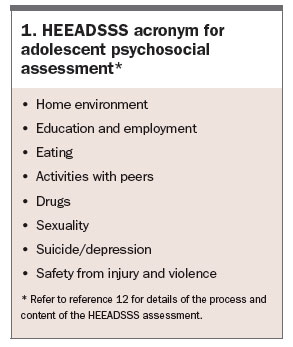
One acronym used to recall other important items in the psychosocial history is HEEADSSS (Box 1).12 In addition, the authors find it helpful to ask the young person and their carers what they think or worry might be the cause of pain, and what they have already found on their internet searches. Accepting that they will explore multiple information sources and welcoming this discussion improves engagement and creates opportunity to prevent harm.
{kind=link}
Physical examination
The presenting history should guide a focused physical examination. In addition to standard examination of the relevant body part(s) or system:
- ask the young person to indicate the location of pain in the exposed body part
- perform sensory testing
– skin: test response to soft-touch (cotton ball, brush), cold (alcohol wipe) and punctate/sharp as a minimum. Add vibration and position sense as indicated
– deep tissues: test response to deep palpation as tolerated
– joint movement: test sensory response to active and passive movement
- map any areas of reduced and/or increased (unpleasant or painful) sensation evoked by the examination
- for limb pain, note any differences between limbs (e.g. colour, temperature, swelling, sweating or trophic changes) that might suggest complex regional pain syndrome (Box 2).13,14
{kind=link}
If abnormal sensation is reported, its location should be compared with the territory of neural structures – cord, roots, plexus, peripheral nerves and their branches. Importantly, abnormal sensation that does not fit with a discrete neural lesion should not be discounted. This may occur due to neural plasticity. The abnormal sensation in the painful area can be used to help patients understand that their pain signalling system may be sending inaccurate signals (e.g. use language such as ‘it is the same harmless cotton wool in both places, so this painful signal is inaccurate’ or ‘this area is sending a pain signal that is not correct, it is not detecting something that is actually harmful’). This can be a light-bulb moment for a young person with persisting pain. Ideally show their parents as well and explain what you have (or have not) found.
Red flags
The sensitivity of clinical red flags to detect serious conditions causing pain in adolescents is uncertain. Nevertheless, it is prudent to screen for general and specific indicators of serious conditions (Table 2).15-17 If red flags are present, diagnostic curiosity, investigations and specialist opinion may be needed. Even if investigations prove normal, vigilant monitoring for change is advisable.
{kind=link}
Investigations
Recommending laboratory and imaging investigations in adolescents with specific pain presentations is beyond the scope of this article. If investigations are warranted, it is important to discuss the rationale, process and results with the adolescent.
Adolescents are generally keen to understand their bodies, so showing them their images while explaining the meaning of reports is a great foundation for further therapeutic discussions. If appropriate, explain that no further investigations are warranted, and that results confirm that it is safe to proceed with the management plan. This can reduce unnecessary and potentially harmful investigations and expedite care.
Explanation
Young people may be hesitant to ask questions so GPs may have to anticipate their information needs. The most frequently asked questions by adolescents in the authors’ experience are:
- Do you believe me?
- Why have I got this pain?
- Is it going to go away/get better?
- Will I be able to do what I want to – socialise, play, study, compete, work?
- Will you help me?
Explain the diagnostic formulation in terms and depth that meet the young person’s needs. Equally important is confident explanation of how other serious causes have been excluded. If the diagnosis is uncertain, be honest and undertake to continue considering the diagnosis while monitoring progress. Checking parental understanding and questions is equally important if they are involved in supporting the young person.
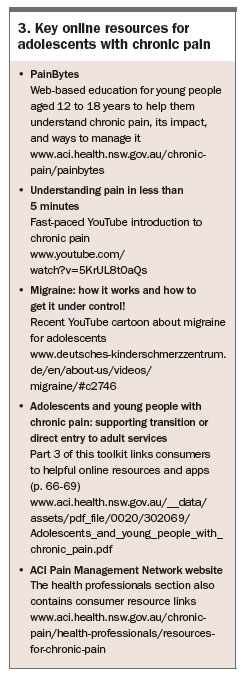
Referring adolescents and families to web-based information should supplement rather than replace a tailored explanation (Box 3). Adolescents and parents should be cautioned about the huge variation in reliability of online pain information. Information about pain in older adults may not apply to young people; for example, prognosis is usually more optimistic in youth.
{kind=link}
Treatment
Definitive treatment of an underlying disorder may be available for some presentations. For the majority, however, a pain rehabilitation approach will be needed. Medications may provide a window of opportunity during which other more sustainable therapies can be progressed. In addition to advice about pain, general advice to promote health and wellbeing should also be offered.
Health promotion
Young people are under-represented in GP consultations, so a presentation of pain creates a rare opportunity to promote health at a time when motivation to change may be high. Offer information and/or interventions to address any of the following areas that are relevant to the young person’s pain experience:
- sleep: if pain is affecting sleep initiation, maintenance or quality, a young person may welcome advice about sleep (www.betterhealth.vic.gov.au/health/healthyliving/teenagers-and-sleep?viewAsPdf=true, www.betterhealth.vic.gov.au/health/conditionsandtreatmentssleep-hygiene?viewAsPdf=true)
- screen time: if more than two hours per day, address in terms of impact on sleep, posture, fitness and pain (http://healthywa.wa.gov.au/Articles/S_T/Screen-time)
- physical activity: set goals consistent with activity guidelines (Australia's physical activity and sedentary guidelines)
- overweight/obesity: offer at least a brief intervention (www.eatforhealth.gov.au)
- smoking and drugs
- mental health
- safety and child protection issues
- school attendance and its therapeutic benefits (www.aci.health.nsw.gov.au/chronic-pain/painbytes/pain-and-school)
Medications
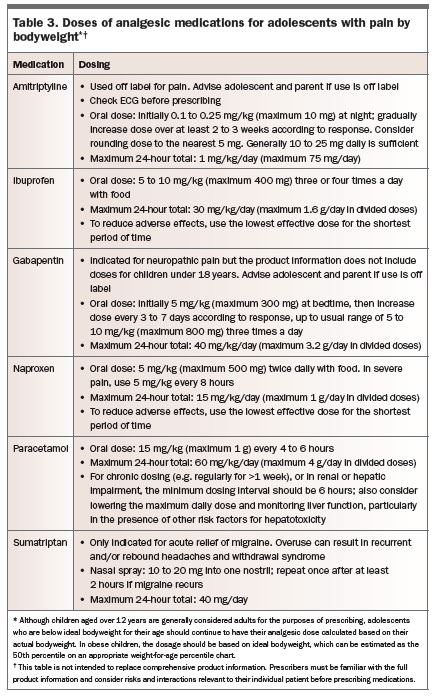
Analgesics may be indicated if pain interferes with sleep, self-care and learning. A tricyclic antidepressant or anticonvulsant may be considered if there is evidence of neuropathic pain. Although no medications are licensed for neuropathic pain in people younger than 18 years, there are consensus guidelines on dosing of amitriptyline and gabapentin for neuropathic pain in children and adolescents.18 Evidence of long-term analgesic efficacy and harms is lacking in young people, so medications with the highest therapeutic index for the shortest possible time should be used.
It is acknowledged that young people with some chronic medical illnesses, such as some rare diseases with a high burden of pain, may require ongoing use of medications, including opioids.19,20 However, even if attending a children’s complex pain service, most adolescents are never prescribed opioids (86%) or have short-term prescription only (8%), with only 2% receiving continuing prescription for chronic severely painful conditions outside the palliative care context.20
Refer to the Therapeutic Guidelines and the Australian Medicines Handbook Children’s Dosing Companion for licensed indications and dosing in younger adolescents.18,21 Dosing advice for more commonly prescribed analgesic medications is provided in Table 3 for easy reference.
Before initiating medication:
{kind=link}
- inform the adolescent and their parents about the rationale, benefits, potential adverse effects, interactions with over-the-counter medications and alternatives. If a tricyclic antidepressant or an anticonvulsant is prescribed, ensure information about suicide risk is sensitively highlighted and discuss a risk-management plan
- agree on medication goals (i.e. what level of pain score reduction, improved function and improved mood would make the medication worthwhile); if this is not achieved, agree that the medication will be stopped
- set a timeframe for review and expected dose reduction and cessation
- discuss safe storage including importance of not carrying medications in
- school bag, and secure storage if
- young children or depressed persons share the home
- counsel learner and provisional drivers, and those involved in potentially dangerous work, about any medication effects on cognition and response times, and their responsibilities while taking the medication
- counsel females of childbearing age about any risks in pregnancy and offer advice on managing this risk.
Psychological therapies
Psychological therapies include neurophysiology education, relaxation, cognitive coping strategies and parenting skills training. A Cochrane review reported that psychological therapies delivered face-to-face are effective for reducing pain intensity in young people with chronic headache, recurrent abdominal pain and musculoskeletal pain, and have a long-lasting effect for reducing disability in headache.22 These therapies may also be delivered individually via telephone, computer program or internet, or as part of multidisciplinary group programs at children’s or adults’ specialist pain services.
In addition to pain-focused therapy, psychologists assess and manage the impact of pain on the adolescent’s sleep and mood, and can help address background mental health and trauma that might influence the pain experience. As these therapies take multiple sessions and interval practice, therapy should be provided as close to home as possible.
Physical therapies
Unless pain is caused by a serious injury or inflammatory illness, rest and passive therapies such as immobilisation, taping, massage or ultrasound are unhelpful and may delay recovery of function. Instead, the role of the physical therapist is to help the adolescent and family learn and co-ordinate physical rehabilitation. This may involve help with tailoring advice about goal setting, graded reactivation and school reintegration to the young person’s activity preferences and abilities. A physiotherapist, occupational therapist, hand therapist, and/or exercise physiologist may fill this role depending on skillset needed and availability.
Complementary therapies
It is common for young people and parents to explore complementary and alternative therapies. Since evidence on effectiveness of these therapies is lacking or poor,23 it can be helpful to counsel families on how to be savvy consumers, including empowering them to ask questions about potential harms, and encouraging them to set therapeutic goals, timeframes and financial limits.
Role of the GP and when to refer
Young people with pain benefit from having a consistent GP or general practice. GPs co-ordinate diagnostic investigations and opinions, and help navigate complex medical and allied health systems. If pain is short lived or not affecting function, assessment and advice to remain active may be sufficient. However, if the young person’s self-management resources are not enough, GPs should refer early to community or private allied health providers. Referral of an adolescent to a specialist multidisciplinary pain management service is indicated when pain:
- lasts more than three months or is
- certain to be chronic from the outset
- interferes with sleep, self-care, mobility or school/work attendance
- has a significant impact on mood and social functioning
- is not improving with treatment by GP and local allied health resources
- context is so complex as to require tight interdisciplinary communication.
Adolescents younger than 16 years of age should be referred to children’s multidisciplinary pain services. Adolescents aged 16 to 18 years may be accepted by children’s services in some states and territories but not in others (e.g. NSW). Once accepted, the young person will be managed by the children’s service and transitioned at an appropriate time (if still needed) to adult services by their 19th birthday.
Young people 18 years and older (or 16 years and older in NSW) should be referred directly to an adult service. A small minority of adolescents who have not yet reached this age, but are living out of home and independent, may also be considered suitable for referral to an adult service. Services and referral criteria can be located at www.apsoc.org.au/facility-directory.
Role of transition services
Transition services, usually associated with tertiary children’s hospitals, help specialist teams prepare young people with complex health conditions for the transition from paediatric to adult services. Transition co-ordinators in some jurisdictions also accept self-referrals and GP referrals. Young people do not have to have seen specialist children’s services to benefit from this support. Referral should be considered if:
- the adolescent is 14 to 25 years of age with a chronic condition/disability
- complex care involving multiple
- specialist providers is required
- there are frequent unplanned hospital admissions
- the adolescent is not adhering to treatment or there is inconsistent clinic attendance
- there are complex psychosocial issues such as financial hardship, family problems, social isolation, unemployment or school absenteeism.
In the absence of complicating factors, this service should be offered to Aboriginal and Torres Strait Islander young people and those from culturally and linguistically diverse backgrounds as a potential means of closing the gap in health outcomes for these groups.
Summary
Chronic pain during adolescence interrupts learning and vocational trajectories and is associated with high emotional burden, social stigma, isolation and disadvantage. There is evidence that health in adolescence and young adulthood is a major determinant of health later in life.24 Health behaviours adopted in adolescence often persist into later adult life. Effective pain management during youth stands to reinstate health and vocational potential, thereby reducing the incidence, burden and cost of pain in later adulthood. GPs and transition co-ordinators can support young people to access and stay with the care they need.PMT
References
- Australian Institute of Health and Welfare. Young Australians: their health and wellbeing 2011. Cat. no. PHE 140 Canberra: AIHW; 2011.
- Cave L, Fildes J, Luckett G, Wearring A. Mission Australia’s 2015 Youth Survey Report. Mission Australia; 2015.
- King S, Chambers CT, Huguet A, et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain 2011; 152: 2729-2738.
- Swain MS, Henschke N, Kamper SJ, Gobina I, Ottová-Jordan V, Maher CG. An international survey of pain in adolescents. BMC Public Health 2014; 14: 447.
- Blyth FM, Van Der Windt DA, Croft PR. Chronic disabling pain: a significant public health problem. Am J Prev Med 2015; 49: 98-101.
- Blyth FM, March LM, Brnabic AJM, Jorm LR, Williamson M, Cousins MJ. Chronic pain in Australia: a prevalence study. Pain 2001; 89: 127-134.
- O’Sullivan PB, Beales DJ, Smith AJ, Straker LM. Low back pain in 17 year olds has substantial impact and represents an important public health disorder: a cross-sectional study. BMC Public Health 2012; 12: 100.
- Henderson JV, Harrison CM, Britt HC, Bayram CF, Miller GC. Prevalence, causes, severity, impact, and management of chronic pain in Australian general practice patients. Pain Medicine 2013; 14: 1346-1361.
- Britto MT, Slap GB, DeVellis RF, et al. Specialists understanding of the health care preferences of chronically ill adolescents. J Adolesc Health 2007; 40: 334-341.
- Dell’Api M, Rennick JE, Rosmus C. Childhood chronic pain and health care professional interactions: shaping the chronic pain experiences of children. J Child Health Care 2007; 11: 269-286.
- Carter B, Lambrenos K, Thursfield J. A pain workshop: an approach to eliciting the views of young people with chronic pain. J Clin Nurs 2002; 11: 753-762.
- Klein DA, Goldenring JM, Adelman WP. HEEADSSS 3.0: The psychosocial interview for adolescents updated for a new century fueled by media. Contem Pediatr 2014; 16-28. Available online at: www.trapeze.org.au/sites/default/files/2014_01_Klein_Goldenring_HEEADSSS3.0_Contemporary %20Pediatrics.pdf (accessed April 2017).
- Harden RN, Bruehl S, Perez RS, et al. Validation of proposed diagnostic criteria (the ‘Budapest Criteria’) for complex regional pain syndrome. Pain 2010; 150: 268-274.
- Merskey H, Bogduk N, eds. Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms, 2nd edition. Seattle: IASP Press; 1994.
- Gray L. Chronic abdominal pain in children. Aust Fam Physician 2008; 37: 398-400.
- Sixsmith E, Starr M. Managing childhood migraine. Aust Fam Physician 2015; 44: 356-359.
- McGrath PJ, Stevens BJ, Walker SM, Zempsky WT, eds. Oxford Textbook of Paediatric Pain. Oxford: Oxford University Press; 2014.
- Australian Medicines Handbook, Children’s Dosing Companion. Adelaide: Australian Medicines Handbook Pty Ltd; 2017.
- WHO guidelines on the pharmacological treatment of persisting pain in children with medical illnesses. Geneva: World Health Organization; 2012.
- Kepreotes EA, Lord SM. Retrospective review of consecutive cases of paediatric complex pain in a New South Wales tertiary children’s hospital. J Paediatr Child Health 2017; (in press).
- Analgesic Expert Group. Pain in children. In: Therapeutic Guidelines – Analgesic. Version 6. Melbourne: Therapeutic Guidelines Ltd; 2012, pp. 143-180.
- Eccleston C, Palermo TM, Williams AC, et al. Psychological therapies for the management of chronic and recurrent pain in children and adolescents. Cochrane Database of Systematic Reviews 2014, Issue 5. Art. No.: CD003968.
- Tsao JC, Zeltzer LK. Complementary and alternative medicine approaches for pediatric pain: a review of the state-of-the-science. Evid Based Complement Altern Med 2005; 2: 149-159.
- Burt MR. Reasons to invest in adolescents. J Adol Health 2002; 31: 136-152.
COMPETING INTERESTS: None.