Assessing and managing IgE-mediated food allergies in children

Dr Joshi is a Staff Specialist at The Children’s Hospital at Westmead; and a Consultant Paediatric Allergist/Immunologist in private practice in Sydney. Dr Frith is a Staff Specialist at Sydney Children’s Hospital; and a Consultant Paediatric Allergist/Immunologist in private practice in Sydney, NSW.
Food Allergy
Allergy
The incidence of food allergy, and particularly peanut allergy, has increased substantially in Australia over the past decade. A thorough clinical history and specific testing should be conducted to identify the allergen. Allergen avoidance and education are currently the mainstays of treatment.
- More than one-third of children with IgE-mediated food allergy will react on their first known ingestion of a food.
- Cow’s milk, egg, peanut, tree nuts, fish, shellfish, soy and wheat cause more than 90% of food allergies in children.
- Exclusion diets should only be undertaken with specialist advice because they may inadvertently worsen, rather than aid, the child’s situation.
- Foods already tolerated in the child’s diet should not be removed if a skin prick test or serum-specific immunoglobulin E to that food is positive but there are no clinical signs of allergy to that food.
- New evidence suggests that early introduction and regular ingestion of certain allergenic foods significantly reduces the risk of developing food allergy.
- There is currently no scientific evidence to suggest anaphylaxis can occur from skin contact with an allergen.
Picture credit: © Astier/BSIP/SPL
Food allergy is an increasingly common problem that affects about one in 10 babies (up to 12 months old) in Australia.1 Furthermore, the incidence of peanut allergy has undergone a 100% increase over the past 10 years.2,3
The mainstays of treatment of children with immunoglobulin E (IgE)-mediated food allergy are correct allergen identification and avoidance, education about management of an acute reaction and optimal treatment of other atopic conditions, particularly asthma. Future treatments may include oral desensitisation. This article discusses IgE-mediated food allergy in children and strategies for its management.
Defining food allergy
A food allergy is an adverse reaction to a generally harmless substance within a food (usually a protein) that is mediated by the immune system. There are essentially three main types of food allergy: IgE-mediated, nonIgE-mediated, and mixed IgE- and nonIgE-mediated. Food may also cause symptoms through nonimmune mechanisms such as lactase deficiency, but this is not defined as a food allergy.
Why is food allergy increasing?
The two main factors that influence the development of allergies are:
- genetics
- the environment.
It seems unlikely that the genetic make-up of humans would have changed significantly in the past 10 to 15 years, so genetic changes do not account for the increase in childhood allergy over this time.
Although there are several theories that have been studied in relation to the increase in food allergy, the hygiene hypothesis is one of the most commonly cited. However, it seems unlikely that a single factor would account for the complexities of these diseases.
Recent studies have suggested a role of exposure to endotoxins from farm animals in both pregnancy and early childhood as a protective factor against developing allergies.4 It may be that the early response of the immune system to these endotoxins decreases the likelihood of developing an atopic response. Changes to our diet and food processing methods may potentially be a factor in the rise in food allergy. Thermal food processing techniques may inadvertently increase the allergenicity of certain foods; for example, roasted peanuts are more allergenic than raw or boiled peanuts. Also, the type and diversity of the gut microbiota and the timing of exposure to an allergen, as well as the route of initial exposure (e.g. gut versus epicutaneous), are under intense study.
Foods implicated in food allergies
- More than 90% of food allergies in children are caused by cow’s milk, egg, peanut, tree nuts, fish, shellfish, soy and wheat.5
- It is important to note that any food is potentially allergenic. In adults, most food-related anaphylaxis is caused by peanut, tree nuts or seafood.6
- Cow’s milk and egg are also implicated as leading causes of anaphylaxis in young children.7,8
IgE-mediated food allergy
IgE-mediated food allergy refers to immediate-type hypersensitivity reactions that occur because specific IgE against that particular allergen is produced. Theoretically, on first exposure to the allergen, the body recognises this protein as foreign and plasma cells produce IgE directed against the allergenic component of that protein. The IgE then sits on the surface of mast cells that are located in various tissues of the body including the skin, the lining of the lungs and mucosa.
On next exposure, the allergen cross-links the specific IgE molecules, resulting in the mast cells releasing granules containing several inflammatory mediators including histamine. These mediators act on the end organs, including blood vessels, bronchioles and mucosal tissues, resulting in the symptoms and signs of an acute allergic reaction. More than one-third of children with IgE-mediated food allergy will react on their first known ingestion of a food, and sensitisation may have occurred via the skin, particularly in infants with a break down in skin barrier function such as with eczema.9-11
Oral allergy syndrome or pollen-food syndrome (IgE-mediated)
Some patients with seasonal allergic rhinitis/conjunctivitis experience itch and irritation of the tongue, mouth and throat after ingestion of some fresh fruits and vegetables. Most of these patients are allergic to cross-reactive proteins common to some pollen and foods, and the condition is known as oral allergy syndrome or pollen-food syndrome. Treatment of patients with this condition involves either avoiding the food or eating it in the cooked form only (if tolerated).
Diagnosing IgE-mediated food allergy
Most cases of IgE-mediated food allergy are fairly easy to recognise. Symptoms generally appear within 30 minutes of ingesting the allergenic food (although they may start up to two hours later) and can occur on the first known exposure to that food. Most food allergic reactions are relatively mild. The symptoms and signs of a mild-to-moderate allergic reaction may include one or more of the following: urticaria, lip and/or mouth swelling (angioedema), vomiting, diarrhoea, abdominal pain and/or acute rhinitis.
Signs of a severe allergic reaction or anaphylaxis may include one or more of the following: difficulty breathing, noisy breathing, swelling of the tongue, swelling and/or tightness in the throat, difficulty talking, a hoarse voice, wheeze, a persistent cough (sometimes described as staccato), loss of consciousness and/or collapse (Box 1). Affected young children may become pale and floppy (a sign of hypotension). More than 90% of children will have cutaneous symptoms before they develop more severe symptoms; however, the reaction can evolve very rapidly. The diagnosis may be less obvious when the trigger food is not easy to identify on history or the symptoms are less defined (Box 2).
{kind=link}
{kind=link}
As food allergy is rarely a trigger for chronic rhinorrhoea, in general, foods should not be removed from the diet in order to treat rhinitis.
It is also important to note that babies have delicate skin and as such, perioral erythema is most likely to be due to contact irritation. Foods such as concentrated tomato and citrus fruits may irritate the skin, especially when the infant self-feeds. This is not a food allergy.
Atopic dermatitis and food allergy
Food allergy does not cause atopic dermatitis but may be co-associated. Evidence would suggest that only up to 50% of children with moderate-to-severe atopic dermatitis have a true food allergy.12,13 Delayed reactions to foods can occur in patients with atopic dermatitis and are not primarily IgE-mediated.
A short period of elimination of potentially allergenic foods may be trialled by specialists in conjunction with dietitians in a minority of patients. However, these diets are difficult and may not yield results. Severe allergic reactions have been reported on re-exposure of children to foods removed from their diet for prolonged periods of time. Therefore, exclusion diets should only be undertaken with specialist advice because they may inadvertently worsen, rather than aid, the child’s situation.
In managing children with atopic dermatitis, treating the underlying skin disorder with emollients and appropriate topical corticosteroids is the most important intervention, not removal of foods.
Investigating food allergy
There are several tests available for identifying the likely cause of a food allergy.
Skin prick tests
Skin prick tests have the advantage of being more sensitive than blood tests for allergen-specific IgE and are the first-line investigation for most immunologists/allergists in Australia. They provide immediate results, are usually well tolerated and rarely cause severe side effects. If an allergy to a fruit, vegetable or processed food is suspected, it is helpful for the patient to bring a sample of that food to the specialist appointment for fresh food testing. Antihistamines should be stopped for three to five days before testing.
Skin prick tests can be performed in patients of any age but require careful interpretation in young infants. The risk of a more severe reaction to a skin test is higher in a young baby (under 12 months).14 Skin prick testing has no role in confirming suspected reactions to food additives or food intolerances.
Blood tests for allergen-specific IgE
Enzyme and fluorescent-based assays called ‘in vitro-specific IgE testing’ or ‘serum-specific IgE testing’ (ssIgE) has replaced the radioallergosorbent test (RAST). If skin prick testing is not available, there is no clear skin on which to perform the test or the patient cannot stop taking their antihistamines, an ssIgE test may be useful.
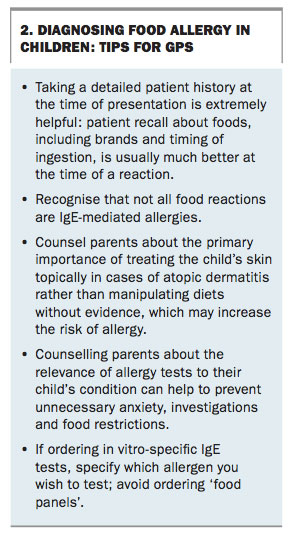
Testing of specific antigens should be ordered rather than ‘food panels’. Results of food panels are confusing and parents often think that all the foods in the panel are to be eliminated from the diet if a result is positive. This can lead to unnecessary and potentially dangerous restrictions.
Allergen component-resolved diagnostic testing (CRD) is relatively new. It uses purified or recombinant allergens (rather than a crude extract of the food) to identify the specific molecules causing sensitisation.15 The value of these tests in Australia still needs to be carefully studied and, therefore, they are not recommended by the authors for routine allergy testing by GPs. They may be used in the specialist setting in some cases.
It is important to note that the magnitude of a skin test reaction or ssIgE result correlates with the likelihood of the patient having a clinical allergy to that food, not with the severity of the reaction. A positive skin test or ssIgE signifies allergic sensitisation and not necessarily clinical allergy.
Tests for IgE-mediated food allergy should be ordered and interpreted alongside a detailed clinical history. In general, foods already tolerated in the diet should not be removed, even if a skin prick test or ssIgE to that food is positive.
Total IgE levels
The total IgE value is often raised in people with allergies and or eczema. However, measurement of the total IgE level does not help in the diagnosis of a food allergy.
Oral food challenges
The gradual feeding of a test food under close supervision, with observation as to whether it is tolerated, is sometimes performed to prove a diagnosis of food allergy when the history is not entirely clear. An oral food challenge may also be used to determine if a food allergy has resolved. Oral food challenges must always be performed by experienced clinicians who have the ability to recognise and manage a patient with anaphylaxis. Extensive resuscitation equipment should be readily available.
Unproven methods
Examples of unproven methods of assessing food allergy include cytotoxic food testing, kinesiology, Vega testing, electrodermal testing, pulse testing, reflexology and hair analysis. These tests have not been scientifically validated and may lead to dangerous avoidance strategies.16
The natural history of food allergy
Most common childhood food allergies resolve before adulthood, although the timing can be variable and difficult to predict. There appears to be a trend to outgrowing allergies at a slower rate.17 Although many children still attain tolerance at a young age, some will take until adolescence to outgrow their allergy, with about 70% achieving tolerance to egg and milk allergens by 16 years of age.17,18 Unfortunately, only about 20% of children will outgrow peanut, tree nut or seafood allergies,19-21 and a number of these may lose their tolerance to the allergen if continued regular exposure to the allergen does not occur.
Allergy prevention
Prevention of allergic disease including food allergy remains an active and evolving area of research. New evidence suggests that early introduction and continued ingestion of allergenic foods significantly reduces the risk of developing food allergy.22,23 The Learning Early about Peanut (LEAP) study demonstrated that in high-risk infants (those with severe eczema and/or an IgE-mediated egg allergy), introduction of peanut before the age of 1 year and regular ingestion reduced the incidence of peanut allergy by 80%.23
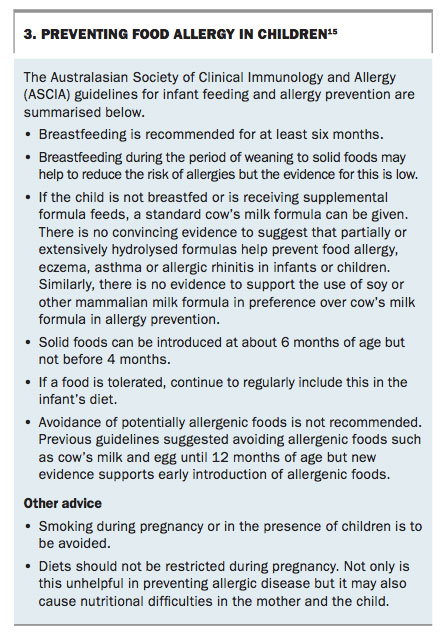
Based on new evidence, the Australasian Society of Clinical Immunology and Allergy (ASCIA) has recently published revised infant feeding guidelines that suggest an approach to preventing food allergy (Box 3).24 Although the guidelines (summarised below) still recommend the introduction of solid foods at about 6 months of age, but not before 4 months, they have changed to actively encourage the introduction of allergenic foods in the first year of life.
{kind=link}
Management of food allergies
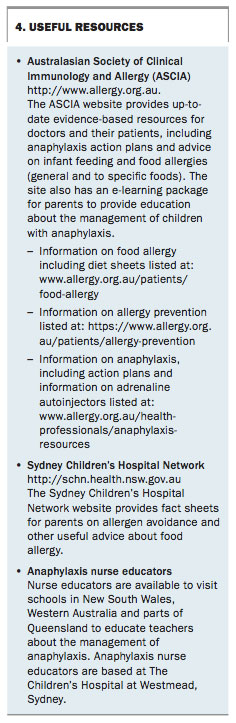
Currently, there is no cure for food allergy and management of affected patients involves avoiding the food allergens. However, accidental ingestions of the allergenic food are not uncommon. Providing clear written information to patients and their families about how to avoid allergens is helpful because food labelling can be confusing. In addition, written action plans to guide the management of children with acute reactions should be provided to patients (dietary information sheets and action plans are available from ASCIA; Box 4).
{kind=link}
Potential pitfalls of food avoidance are nutritional inadequacy and psychological difficulties. If a major staple food such as cow’s milk is removed from a child’s diet, advice from a dietitian is important in order to assess adequate nutritional intake. Children with gross calcium deficiencies and even malnutrition are seen in specialist clinics after being placed on restricted diets.
Box 5 provides some tips for GPs managing children with food allergies.
{kind=link}
Future treatments
Numerous trials are under way around the world seeking a better solution for the management of people with food allergies. These include oral, sublingual, subcutaneous and epicutaneous food immunotherapies, with or without adjuvants.25 Although results are promising, these therapies are not yet ready for clinical use. Many of the patients using these therapies achieve desensitisation, particularly with ongoing consumption of the allergen, but far fewer develop sustained oral tolerance. Optimising oral tolerance while maintaining an acceptable safety profile are the two main barriers to food immunotherapy at present.
Several studies have shown that even in infants with anaphylaxis to cow’s milk or egg, about 70% can tolerate milk or egg in a baked product such as a muffin or cake.1,26-28 This is because the protein is altered by heat and probably because the food matrix has a modifying effect on the allergen absorption. Challenging the allergic child to these allergens should be closely supervised by a specialist. If the baked proteins are tolerated, regular consumption may lead to faster resolution of the allergy. If the child is already tolerating baked egg or milk but has an allergy to the unmodified protein, the baked product should not be removed from their diet.
When to refer
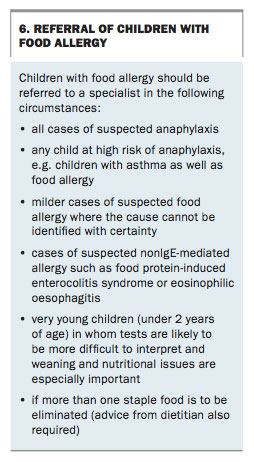
Tips for which patients with food allergies to refer to a specialist are listed in Box 6.
{kind=link}
Anaphylaxis
Fatalities from anaphylaxis are extremely rare. There is currently no scientific evidence to suggest anaphylaxis can occur from skin contact with an allergen.
Risk factors for anaphylaxis
There is no test that can rule out anaphylaxis for a child with food allergy. There are, however, several epidemiological factors that have been found to be associated with anaphylaxis fatalities and/or may favour the provision of the child with an adrenaline autoinjector. There is also increasing evidence that concurrent presence of other atopic diseases is associated with increased severity of signs during a food allergic reaction. These factors include:
- a history of previous anaphylaxis
- asthma
- association with a particular allergen (i.e. peanut or tree nut, especially cashew)
- having a previous significant reaction to a very small amount of that protein
- the child’s age; for example, the risk of fatality is higher in adolescence and young adulthood than at other ages
- lack of access to emergency medical care.
Management of anaphylaxis
Although it is beyond the scope of this article to discuss anaphylaxis management in detail, the first line of management in the acute setting is intramuscular adrenaline 1:1000 at a dose of 0.01 mL/kg to a maximum of 0.5 mL into the lateral thigh. This should be repeated after five minutes if the patient is not improving.
Antihistamines may reduce the skin and gastrointestinal symptoms of an allergic reaction but do not treat or prevent anaphylaxis. Oral corticosteroids are not the first-line treatment for a patient with anaphylaxis.
If a child is considered at risk of anaphylaxis then an emergency adrenaline autoinjector device should be prescribed. There is only one device currently available on the PBS, although other brands are in use in other countries. ASCIA recommends that the lower-dose (0.15 mg adrenaline) junior versions of these devices be prescribed for children weighing between 10 and 20 kg and the higher-dose (0.30 mg adrenaline) devices for individuals weighing more than 20 kg.29 Note that these recommendations differ from the product information for the autoinjectors, which states that the 0.15 mg adrenaline dose versions are intended for children weighing between 15 and 30 kg, and the 0.30 mg adrenaline dose devices for children and adults weighing more than 30 kg. The ASCIA recommendations are closer to the recommended dose of adrenaline that would be given for anaphylaxis if a patient was treated in hospital (e.g. 0.01 mL/kg adrenaline 1:1000, maximum of 0.5 mL).
Conclusion
The rate of food allergy is increasing, as is the rate of anaphylaxis to food. Thankfully most food allergy is mild and fatalities are rare. GPs play a vital role in managing affected patients because they are usually the first to see the child after an allergic reaction. It is important to take a detailed history and to provide this to the specialist if referral is appropriate. Treating co-existing atopic conditions is helpful in the overall management of a child with food allergy. Reassuring parents, providing evidence-based resources and discouraging unsupervised dietary restriction will help optimise the child’s nutritional status. Recognising anaphylaxis and the risk factors can be life-saving. Prescribing adrenaline autoinjectors appropriately and educating parents in using the device is a service that GPs can provide in conjunction with a specialist.
Acknowledgements
The authors would like to thank the Australasian Society of Clinical Immunology and Allergy (ASCIA) for much of the source material regarding anaphylaxis, allergy prevention and unproven testing.
COMPETING INTERESTS: Dr Joshi: None. Dr Frith has received personal fees from Abbott and Nestle Nutrition.
References
- Osborne NJ, Koplin JJ, Martin PE, et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J Allergy Clinical Immunol 2011; 127: 668-676.e1-2.
- Ben-Shoshan M, Kagan RS, Alizadehfar R, et al. Is the prevalence of peanut allergy increasing? A 5-year follow-up study in children in Montreal. J Allergy Clinical Immunol 2009; 123: 783-788.
- Sicherer SH, Munoz-Furlong A, Sampson HA. Prevalence of peanut and tree nut allergy in the United States determined by means of a random digit dial telephone survey: a 5-year follow-up study. J Allergy Clinical Immunol 2003; 112: 1203-1207.
- Ege MJ, Bieli C, Frei R, et al. Prenatal farm exposure is related to the expression of receptors of innate immunity and to atopic sensitisation in school age children. J Allergy Clinical Immunol 2006; 117: 817-823.
- Sampson HA. Food allergy. part 1: immunopathogenesis and clinical disorders. J Allergy Clin Immunol 1999, part 1; 103 (5 Pt 1); 717-784.
- Sicherer S. Epidemiology of food allergy. J Allergy Clin Immunol 2011; 127: 594-602.
- de Silva IL, Mehr SS, Tey D, Tang ML. Paediatric anaphylaxis: a 5 year retrospective review. Allergy 2008; 63: 1071-1076.
- Liew WK, Williamson E, Tang ML. Anaphylaxis fatalities and admissions in Australia. J Allergy Clinical Immunol 2009; 123: 434-442.
- Fox AT, Sasieni P, du Toit G, Syed H, Lack G. Household peanut consumption as a risk factor for the development of peanut allergy. J Allergy Clinical Immunol 2009; 123: 417-423.
- Tan HT, Ellis JA, Koplin JJ, et al. Filaggrin loss-of-function mutations do not predict food allergy over and above the risk of food sensitization among infants. J Allergy Clinical Immunol 2012; 130: 1211-1213.e3.
- Nickolls C, Campbell DE. Top 10 food allergy myths. J Paediatr Child Health 2015; 51: 852-856.
- Martin PE, Eckert JK, Koplin JJ, et al. Which infants with eczema are at risk of food allergy? Results from a population-based cohort. Clin Exp Allergy 2015; 45: 255-264.
- Eigenmann PA, Sicherer SH, Borkowski TA, Cohen BA, Sampson HA. Prevelance of IgE-mediated food allergy among children with atopic dermatitis. Pediatrics 1998; 101: E8.
- Norrman G, Falth-Magnusson K. Adverse reactions to skin prick testing in children - prevalence and possible risk factors. Pediatr Allergy Immunol 2009; 20: 273-278.
- Matricardi PM, Kleine-Tebbe J, Hoffmann HJ, et al. EAACI Molecular allergology user’s guide. Pediatr Allergy Immunol 2016: Suppl 23: 1-250.
- Australasian Society of Clinical Immunology and Allergy (ASCIA). Unorthodox testing and treatment for allergic disorders. Sydney: ASCIA; 2010. Available online at: http://www.allergy.org.au/patients/allergy-testing/unorthodox-testing-and-treatment (accessed February 2017).
- Savage JH, Matsui EC, Skripak JM, Wood RA. The natural history of egg allergy. J Allergy Clinical Immunol 2007; 120: 1413-1417.
- Skripak JM, Matsui EC, Mudd K, Wood RA. The natural history of IgE-mediated cow’s milk allergy. J Allergy Clinical Immunol 2007; 120: 1172-1177.
- Skolnick HS, Conover-Walker MK, Koerner CB, Sampson HA, Burks W, Wood RA. The natural history of peanut allergy. J Allergy Clinical Immunol 2001; 107: 367-374.
- Fleischer DM, Conover-Walker MK, Matsui EC, Wood RA. The natural history of tree nut allergies. J Allergy Clinical Immunol 2005; 116: 1087-1093.
- Tsabouri S, Triga M, Makris M, Kalogeromitros D, Church MK, Priftis KN. Fish and shellfish allergy in children: review of a persistent food allergy. Pediatr Allergy Immunol 2012; 23: 608-615.
- Koplin JJ, Osborne NJ, Wake M, et al. Can early introduction of egg prevent egg allergy in infants? A population-based study. J Allergy Clinical Immunol 2010; 126: 807-813.
- Du Toit G, Roberts G, Sayre PH, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015; 372: 803-813.
- Australasian Society of Clinical Immunology and Allergy (ASCIA). Infant feeding and allergy prevention. Sydney: ASCIA; 2016. Available online at: http://www.allergy.org.au/health-professionals/papers/ascia-guidelines-for-infant-feeding-and-allergy-prevention (accessed February 2017).
- Nurmatov U, Dhami S, Arasi S, et al. Allergen immunotherapy for IgE-mediated food allergy: a systematic review and meta-analysis. Allergy 2017 Jan 6; epub ahead of print: doi:10.1111/all.13124
- Mehr S, Turner PJ, Joshi P, Wong M, Campbell DE. Safety and clinical predictors of reacting to extensively heated cow’s milk challenge in cow’s milk-allergic children. Ann Allergy Asthma Immunol 2014; 113: 425-429.
- Turner PJ, Mehr S, Joshi P, et al. Safety of food challenge to extensively heated egg in egg-allergic children: a prospective cohort study. Pediatr Allergy Immunol 2013; 24: 450-455.
- Leonard SA, Caubet JC, Kim JS, Groetch M, Nowak-Wegrzyn A. Baked milk and egg containing diet in the management of milk and egg allergy. J Allergy Clin Immunol Pract 2015; 3: 13-23.
- Australasian Society of Clinical Immunology and Allergy (ASCIA). ASCIA guidelines – adrenaline (epinephrine) autoinjector prescription. Sydney: ASCIA; 2016. Available online at: http://www.allergy.org.au/health-professionals/anaphylaxis-resources/adrenaline-autoinjector-prescription (accessed February 2017).