Galactorrhoea and mildly elevated prolactin levels: what is the cause?

Pituitary disorders
This case describes a woman with galactorrhoea associated with hyperprolactinaemia. Although there are many physiological, pathological and pharmacological causes of hyperprolactinaemia, many of these can be excluded following a detailed history and physical examination.
- In women with galactorrhoea and a mildly elevated serum prolactin level, a history of normal menstruation indicates that a clinically significant pituitary tumour is unlikely.
- Pituitary MRI and complete pituitary function tests do not need to be routinely performed in this situation.
- Hyperprolactinaemia is present in less than 50% of women with galactorrhoea and normal menstruation.
- Many causes of hyperprolactinaemia can be excluded following a detailed history and physical examination.
Case scenario
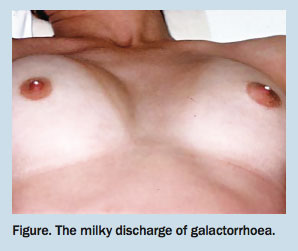
A 36-year-old woman presents with an eight-week history of a white discharge from both nipples (Figure). It was first noted when bathing and she has subsequently been squeezing her breasts each morning under the shower. She believes that the discharge is getting worse.
{kind=link}
Her menstrual periods are regular occurring every 28 days and lasting for five days. There is no history of persistent headaches or visual complaints, and pregnancy and lactation have been excluded. She is married and has an 8-year-old son. She has a history of depression and has recently commenced an exercise program to improve her overall fitness.
Her serum prolactin level is 940 mIU/L (reference range, 50 to 500 mIU/L), with a repeat measurement that was serially diluted in a different laboratory at 723 mIU/L (reference range, 85 to 319 mIU/L).
What is galactorrhoea and how is it caused?
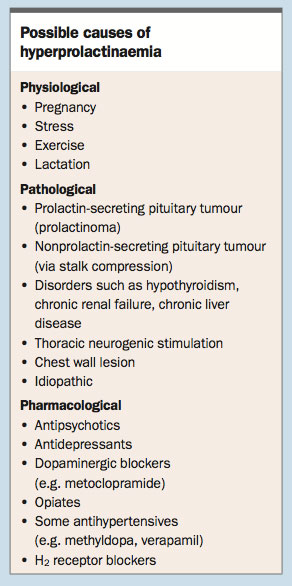
Galactorrhoea is defined as a nonpathological nipple discharge unrelated to pregnancy or lactation. It is caused by either increased stimulation of the mammary gland associated with high circulating levels of prolactin or an increased affinity of prolactin receptors in the mammary gland associated with circulating prolactin levels within the reference range. Hyperprolactinaemia is present in less than 50% of women with galactorrhoea and normal menstruation.1 The causes of hyperprolactinaemia can be physiological, pathological or pharmacological (Box).
{kind=link}
Does the case history give any clues to the possible causes of galactorrhoea?
The case history excludes pregnancy and lactation. The serum prolactin level is only about twice the upper limit of normal, therefore, several causes of hyperprolactinaemia (e.g. a macroprolactinoma) can be excluded.
It is important to note that, although the reference range quoted by the first pathology laboratory was 50 to 500 mIU/L, some laboratories quote the upper limit as 350 mIU/L and others up to 750 mIU/L. The reason for this is, in contrast to many other hormones (e.g. thyroxine), circulating prolactin levels are not distributed in a Gaussian manner (i.e. bell shaped) and there is a skew distribution. Most values are towards the lower part of the reference range and only a few ‘normal’ people have values in the higher range. The upper limit of the quoted reference range depends on whether the laboratory has determined the cut-off as two standard deviations above the mean (appropriate for hormones with Gaussian distributions, thus including 95% of the normal population in the reference range whereas 2.5% of the normal population will have values above and below that range) or whether the cut-off for the upper limit is taken to incorporate the lowest 97.5% of the normal population. Thus a serum prolactin level of 700 mIU/L in a laboratory that quotes the upper limit of normal at 400 or 500 mIU/L may, in reality, be ‘normal’.
The patient’s regular menstruation excludes any clinically significant cause for hyperprolactinaemia (such as a prolactinoma).
Daily squeezing of breasts results in nipple stimulation and this neurogenic activation can lead to a reduced production of dopamine (a prolactin-inhibitory factor) by the hypothalamus causing increased prolactin secretion from the lactotrophs in the anterior pituitary (the same mechanism as with suckling).
Although a lack of headaches or visual complaints does not exclude a large pituitary tumour, the presence of these symptoms should make you suspicious of this pathology.
There was no mention of drug therapy during the case presentation but in view of the patient’s history of depression, it would be important to clarify if she is taking an antidepressant. She had recently commenced an exercise program therefore possible nipple stimulation associated with jogging without breast support (neurogenic mechanism) could also be a factor.
Does an elevated serum prolactin level less than twice the upper limit of normal give a clue to the aetiology?
Absolutely. As mentioned above, a macroprolactinoma can be excluded because the serum prolactin level would generally be at least 20 times the upper limit of normal. A microprolactinoma is also quite unlikely because the prolactin level would usually be significantly higher. An increase in prolactin levels of this magnitude is consistent with drug therapy, hypothyroidism, chronic renal failure, chronic liver disease, stress, pituitary stalk compression from a macroadenoma (leading to reduced dopamine levels resulting in increased prolactin secretion from the pituitary lactotrophs), and repeated nipple stimulation or other forms of thoracic neurogenic stimulation. The current US Endocrine Society clinical practice guideline recommends excluding medication use, renal failure, hypothyroidism and pituitary and parasellar tumours in patients with symptomatic nonphysiological hyperprolactinaemia (overall high-quality evidence).2
Case continued
A more detailed history indicates that the patient has been taking clomipramine for the past three months for depression. She wears a sports bra when jogging so nipple stimulation while exercising is not likely to be relevant. There are no clinical features to suggest hypothyroidism, chronic renal failure or chronic liver disease. Serum thyroid-stimulating hormone and creatinine levels as well as liver function tests are all normal. Her weight has been stable and there are no clinical features to suggest hypopituitarism. Visual fields are normal to confrontation.
Should a pituitary MRI be performed?
In this particular case, after counselling the patient, I would choose not to initially image the pituitary gland. In rationale, a macroprolactinoma has been excluded as the serum prolactin level is not sufficiently high. Pituitary stalk compression is also extremely unlikely because of regular menses and no other clues to suggest a macroadenoma (functioning or nonfunctioning). Even if an MRI is performed and it reveals a microadenoma, it would be difficult to exclude an incidentaloma as about 10% of patients undergoing radiological investigation for nonpituitary disorders have clinically unsuspected pituitary tumours, mostly less than 10 mm in diameter.3
However, the decision on whether to perform an MRI of the pituitary gland in this particular clinical case may be considered controversial. In a symptomatic patient with suspected drug-induced hyperprolactinaemia, the US Endocrine Society clinical practice guideline suggests discontinuation of the medication for three days or substitution of an alternative drug, followed by remeasurement of serum prolactin levels.2 Discontinuation or substitution of an alternative drug would have to be undertaken after consulting with the patient’s psychiatrist. If the drug cannot be discontinued for medical reasons and the onset of the hyperprolactinaemia does not coincide with therapy initiation, obtaining a pituitary MRI to help differentiate between medication-induced hyperprolactinaemia and symptomatic hyperprolactinaemia due to a pituitary or hypothalamic mass is recommended, but based on low-quality evidence.2
In this woman, the timing of the galactorrhoea and hyperprolactinaemia onset with medication prescribing clearly implicates the antidepressant.
How should this patient be managed?
A clinically significant pituitary tumour has been excluded in this case scenario based on the history, examination and investigations. The most likely cause for the galactorrhoea and mildly elevated prolactin level is the antidepressant treatment with perhaps some contribution from regular nipple stimulation (daily squeezing of her breasts under the shower). The patient should therefore be given a detailed explanation of the underlying pathophysiology and advised to stop squeezing her breasts (thus reducing nipple stimulation). If the galactorrhoea itself is not significantly affecting her quality of life (it is not spontaneous or staining her clothes), then no medication need be prescribed. If the galactorrhoea had been more severe and causing her concern, a dopamine agonist such as cabergoline or bromocriptine could be given. Cessation of the antidepressant would almost certainly result in normoprolactinaemia and resolution of the galactorrhoea, but her psychiatrist may not be keen on this option.
Summary
The investigation and management of a woman with galactorrhoea and a mildly elevated serum prolactin level is presented in this case study. Pituitary MRI and complete pituitary function tests do not need to be routinely performed in this situation, and a history of normal menstruation indicates that a clinically significant pituitary tumour is unlikely.
References
- Kleinberg DL, Noel GL, Frantz AG. Galactorrhea: a study of 235 cases, including 48 with pituitary tumors. N Engl J Med 1977; 296: 589-600.
- Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011; 96: 273-288.
- Anagnostis P, Adamidou F, Polyzos SA, Efstathiadou Z, Panagiotou A, Kita M. Pituitary incidentalomas: a single-centre experience. Int J Clin Pract 2011; 65: 172-177.