Managing the rising burden of chronic liver disease: chronic hepatitis B and C

Hepatitis
Collaboration between community and specialist services is key to managing the increasing burden of chronic liver disease, which may lead to cirrhosis, liver failure and liver cancer. Chronic hepatitis B and C, which account for about 8% of the chronic liver disease in Australia, are discussed in this article.
- Chronic hepatitis B and chronic hepatitis C represent about 8% of all cases of chronic liver disease in Australia.
- The rising prevalence of chronic liver disease contributes to increasing rates of cirrhosis, liver failure and liver cancer.
- Chronic hepatitis B and C can be asymptomatic in the early stages of infection.
- Screening at-risk populations for hepatitis B virus and/ or hepatitis C virus will identify patients who require further management to prevent disease progression.
- Highly effective antiviral treatments are available to treat chronic hepatitis B and chronic hepatitis C.
- Patients with advanced fibrosis or cirrhosis of any cause should be referred to a liver specialist.
Picture credit: © Freshidea/Stock.adobe.com
Chronic liver disease affected more than 6 million people in Australia in 2012 and the prevalence is expected to rise to over 8 million by 2030. 1 Chronic hepatitis B and C together represent about 8% of all cases of chronic liver disease in Australia, with almost half a million people affected. Although less prevalent than nonalcoholic fatty liver disease, chronic viral hepatitis is a common cause of cirrhosis and liver failure, and accounts for 70 to 80% of all cases of hepatocellular carcinoma (HCC).
This article aims to help GPs recognise and diagnose patients with chronic hepatitis B or C in primary care, assess the severity of liver disease using clinical and noninvasive markers, recognise the need to manage comorbidities in patients with chronic liver disease and appropriately refer patients who require specialist assessment and management. Nonalcoholic fatty liver disease and alcoholic liver disease were discussed in a previous article in Medicine Today (January 2017 issue).2
Chronic hepatitis B
Case study 1
Mr CX, a 45-year-old man from China, presents requesting antibiotics for flu-like symptoms of two days’ duration. He is assessed as most likely having an upper respiratory viral illness and antibiotics are deferred. Further history reveals he has no concomitant medical conditions, takes no regular medications and does not drink alcohol. He was born in China and left the country 15 years ago, with his wife and son. He runs the family business, a computer repair shop. His body mass index is 22.5 kg/m2 and his blood pressure is 120/75 mmHg. Cardiovascular and gastrointestinal examinations are normal.
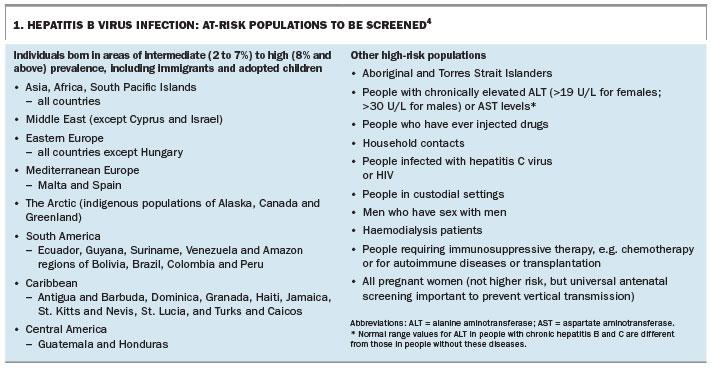
Mr CX comes from a country with a high prevalence of chronic hepatitis B (Box 1). Although he is asymptomatic from the liver point of view, and is presenting to the family GP for a different reason (viral respiratory symptoms), this presentation provides an opportunity to discuss the possible diagnosis and to screen for hepatitis B; the screening is also offered to his wife and son. The patient is encouraged to discuss screening for hepatitis B virus (HBV) infection with his extended family (siblings, parents); education, immunisation, monitoring or treatment would likely be offered to extended family members who test positive. A letter of introduction is provided to the patient to share with extended family members to facilitate this discussion and encourage them to attend their family GPs for testing.
{kind=link}
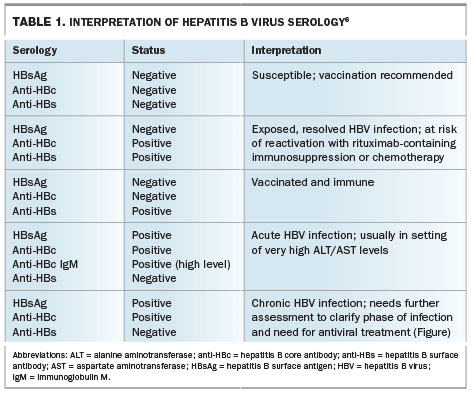
Mr CX returns a week later for a review and to discuss the results of his tests. His flu-like symptoms have resolved completely. Blood investigations show elevated alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels (ALT, 65 U/L [normal range, NR, males <30 U/L]; AST, 54 U/L [NR <35 U/L]) but within normal range levels of gamma glutamyl transferase (GGT; 45 U/L), alkaline phosphatase (ALP; 40 U/L), bilirubin (15 micromol/L) and albumin (39 g/L). The platelet count is 240 x 109/L (NR 150 to 400 x 109/L). HBV serology shows that HBsAg (hepatitis B surface antigen) is positive, HBeAg (hepatitis B envelope antigen) is negative, anti-HBe (hepatitis B envelope antibody) is positive and HBV DNA level is 54,000 IU/mL.
On further questioning, Mr CX recalls that an uncle in China died with ‘yellow jaundice’ and might have had cancer of the liver. The family doctor refers Mr CX for a liver ultrasound examination, which shows a smooth but coarse liver, without additional overt features of cirrhosis, portal hypertension or liver lesion.
What are the next steps?
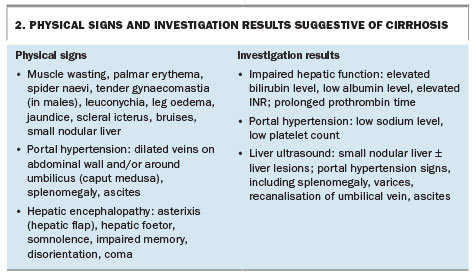
Mr CX has chronic hepatitis B with elevated liver enzyme and HBV DNA levels. The normal platelet count and bilirubin and albumin levels are reassuring that he does not have portal hypertension or decompensated liver disease (Box 2). The coarse liver seen on the liver ultrasound is nonspecific, but in the context of the diagnosis of chronic hepatitis B, this requires further evaluation.
{kind=link}
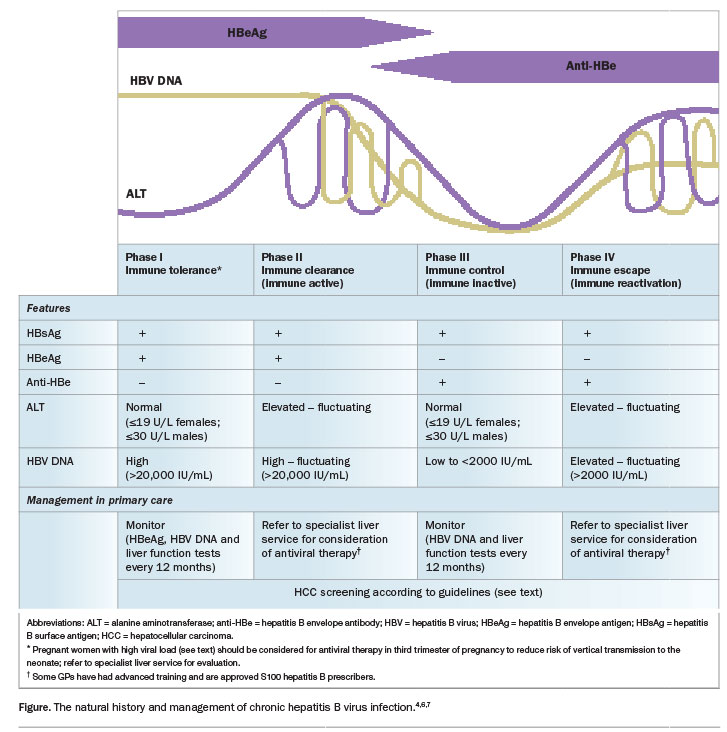
Mr CX is referred to a liver specialist service. The HBV serology, ALT and HBV DNA levels indicate he is in the immune escape (immune reactivation) phase and therefore meets criteria for treatment. The liver specialist performs transient elastography (a FibroScan), which returns an elevated liver stiffness reading of 13.5kPa; this is in the cirrhotic range
(F4, cirrhosis or advanced liver fibrosis). Tenofovir 300 mg daily is prescribed, and Mr CX is advised that this therapy will be lifelong and will reduce his chance of developing liver cancer or liver failure. As recommended by guidelines, he will have six-monthly liver ultrasound examination and alpha-fetoprotein testing for the rest of his life to screen for HCC.3,4
Diagnosis and management
An estimated 218,000 individuals in Australia are infected chronically with HBV, and most of these people were born in countries with intermediate to high prevalences for chronic hepatitis B or are Aboriginal and Torres Strait Islanders.4,5 Chronic hepatitis B is usually asymptomatic, and therefore the diagnosis should be considered in all at-risk groups and opportunistic screening for HBV infection offered (Box 1).4
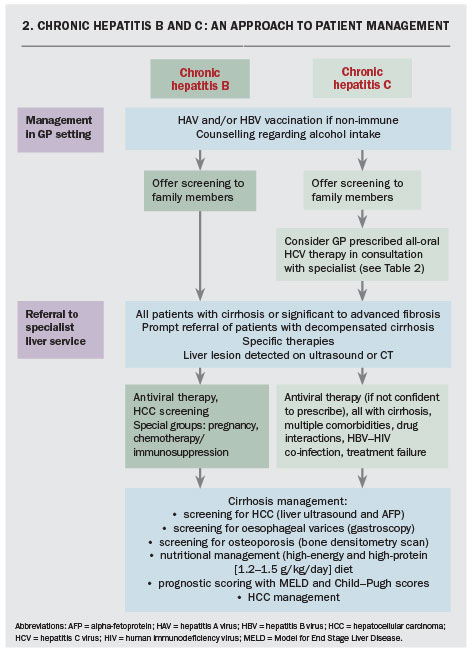
The interpretation of HBV serology is summarised in Table 1 and the natural history and management of chronic HBV infection is shown in the Figure.4,6,7 Specialist referral for antiviral treatment largely is guided by the HBV serology results and HBV DNA and ALT levels.4,7 All patients with cirrhosis should also be referred for specialist management; physical signs and investigation results suggestive of cirrhosis are listed in Box 2. The treatment options for chronic hepatitis B infection include oral nucleot(s)ide analogues (entecavir and tenofovir) and pegylated interferon. Evaluation and management of patients with suspected and confirmed chronic HBV infection is summarised in Flowcharts 1 and 2 and the Figure.
{kind=link}
{kind=link}
{kind=link}
Special considerations
Particular groups of patients with chronic hepatitis B require special consideration.
Patients without cirrhosis
Patients with chronic hepatitis B are at risk of HCC because of a combination of genetic and direct carcinogenic and inflammatory effects of HBV, even before cirrhosis has developed. Surveillance for HCC, with six-monthly liver ultrasound examination and alpha-fetoprotein measurement, should be performed in:3,4
- all patients with cirrhosis and chronic hepatitis B
- patients without cirrhosis who are Asian men aged 40 years or older, Asian women aged 50 years or older or Africans aged 20 years or older, or patients who have a family history of HCC.
Pregnant women with high viral load
Pregnant women with chronic hepatitis B and an HBV DNA (viral load) of 106 IU/mL or higher should be considered for antiviral therapy in the third trimester of pregnancy (from gestational week 28 to 32 onward) to reduce the risk of vertical transmission to the neonate. All HBsAg-positive women with HBV DNA of 106 IU/mL or higher should be referred to a specialist liver service by week 20 of pregnancy to discuss the potential benefits and safety of such an approach during pregnancy, as well as postpartum management of their newborn.
As with all HBsAg-positive women, the newborn should receive HBV immunoglobulin (HBIG) and the first dose of HBV vaccine within 12 hours of birth, and completion of HBV vaccination by the GP according to guidelines.8 Pregnant women who potentially meet HBV treatment criteria independent of their pregnancy should also be referred to specialist services (Figure).
Patients due to undergo chemotherapy or immunosuppressive therapy for malignant, inflammatory or autoimmune conditions
Modulation of the immune system with chemotherapy or immunosuppression in people with concomitant chronic hepatitis B (HBsAg positive) or past exposure to chronic hepatitis B (HBsAg negative, anti-HBc positive) may contribute to HBV reactivation because of the inherent relationship between the Virus and the immune system. This can present clinically as mild biochemical hepatitis through to more severe outcomes of fulminant liver failure and death. The risk of HBV reactivation is associated with the individual’s HBV status and the potency and duration of chemotherapy or immunosuppression.
Patients who will be treated with low-dose corticosteroids (e.g. prednisone for less than one week), intra-articular corticosteroids or traditional immunosuppression (monotherapy) with azathioprine, 6-mercaptopurine or methotrexate are at lowest risk of HBV reactivation (<1%), and can simply be observed in the primary care setting if they otherwise do not meet criteria for specialist referral. Patients receiving longer duration or more potent chemotherapy or immunosuppression should be screened for HBV infection prior to the initiation of chemotherapy or immunosuppression and referred to a specialist liver service for consideration of prophylactic antiviral therapy to prevent HBV reactivation.9,10
Chronic hepatitis C
Case study 2
Ms TT, a 35-year-old woman, attends her family GP as she has heard there are new treatments for hepatitis C. She first presented 10 years ago with fatigue, and after a thorough evaluation was found to have a mildly elevated ALT level (45 U/L, NR females <19 U/L) and to be positive for anti-HCV (hepatitis C virus antibody). Viral serology testing revealed she was negative for anti-HAV IgG (hepatitis A immunoglobulin G antibody), HBsAg anti-HBc (hepatitis B core antibody), anti-HBs (hepatitis B surface antibody) and HIV serology. The family GP administered a course of hepatitis A and B vaccines.
Ms TT’s risk factor for hepatitis C virus (HCV) infection was short-term recreational intravenous drug use 13 years ago, at the age of 22 years. She has mild depression, which is managed with venlafaxine. She takes no herbal therapies or recreational drugs, and drinks about 20 g of alcohol two to three times per week. She is single and works as a bank teller.
She was referred to a liver specialist service 10 years ago; at that time she was suffering significant depression related to a relationship breakup. Potential treatment with pegylated interferon and ribavirin was discussed, but this was deferred in view of her active depression, which could have been exacerbated by interferon.
A follow-up review appointment was scheduled at the liver clinic but she became ‘caught up with life’ and did not return.
What are the next steps?
Ms TT’s chronic HCV infection should be re-evaluated and she should be considered for all-oral HCV antiviral therapy.
The gastrointestinal examination is normal. Results of investigations show ALT 65 U/L (NR <19 U/L), AST 40 U/L (NR <35 U/L), with normal ALP, GGT, bilirubin and albumin levels. The full blood count is normal, and the platelet count is within the normal range (210 x 109 [NR 150 to 400 x 109/L]). The INR is 1.0. The serum creatinine level is
65 µmol/L and estimated glomerular function (eGFR) 90 mL min/1.73m2 (both normal); electrolytes levels are normal. The HCV RNA level is 5.4 x 106 IU/mL and the HCV genotype is 1a. Liver ultrasound results are normal.
A noninvasive assessment of hepatic fibrosis is performed by calculating the AST to platelet ratio index (APRI); this returns a score of 0.544, which is reassuring for the exclusion of cirrhosis. After discussion with the patient, an eight-week course of oral antiviral therapy with once-daily ledipasvir–sofosbuvir (co-formulation) is prescribed. Potential drug interactions with Ms TT ’s antidepressant venlafaxine are excluded by checking the hepatitis drug interactions website ‘HEP Drug Interaction Checker’
(www.hep-druginteractions.org).
Management options for chronic hepatitis C – collaboration between primary care and specialist centres
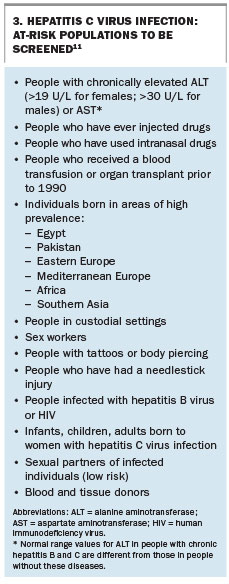
More than 230,000 individuals are affected by chronic hepatitis C in Australia, and in 2012 it was the leading cause of liver failure and liver cancer, contributing to a significant health and economic burden.1 The main risk factor (over 80% of cases) is a history of injecting drug use. At-risk populations who should be screened for HCV infection are listed in Box 3.11
{kind=link}
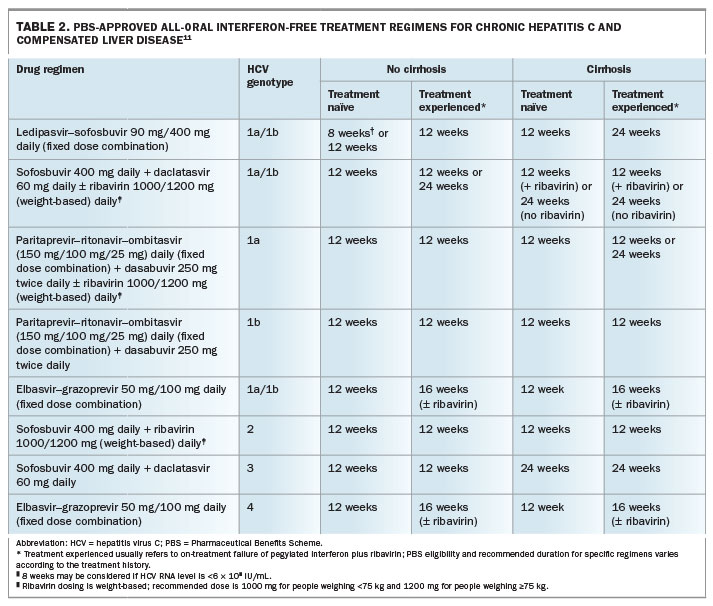
Since March 2016, several all-oral, interferon-free treatment regimens have been listed on the PBS for the treatment of infections with HCV genotypes 1, 2, 3 and 4. These regimens have a tolerable side effect profile and achieve sustained virologic response rates (SVR 12; defined as a negative HCV RNA 12 weeks after completion of therapy) of over 95% after eight to 24 weeks of therapy. It is anticipated that all-oral therapies will soon be available for all patients, regardless of the infecting HCV genotype. The current approved treatment regimens and their indications are summarised in Table 2. A comprehensive guideline on the management of chronic HCVinfection in Australia is provided in the Australian recommendations for the management of hepatitis C virus infection: a consensus statement 2017 and also in a recent article published in Medicine Today.11,12
{kind=link}
The PBS listings of the all-oral antiviral treatments for chronic hepatitis C infection require that they be prescribed by medical practitioners (including GPs) experienced with the treatment of chronic hepatitis C infection, or in consultation with a gastroenterologist, hepatologist or infectiousdiseases physician experienced in the treatment of chronic hepatitis C infection.
The latter stipulation by the PBS allows the opportunity for patients with chronic hepatitis C to be managed by the family GP in addition to by specialists, allowing greater access to treatment for patients across Australia. This is essential, as even with the increased cure rates of the new therapies, a substantial increase in the number of people treated each year will be necessary to effect a significant reduction in HCV prevalence and HCV-related mortality in the long term.13 Furthermore, specific targeting of patient groups with high rates of HCVtransmission (people who inject drugs and prisoners) has a high likelihood of substantially reducing new cases of HCV infection, which will be essential to reduce the future disease burden.
Communication and collaboration between community GPs and local specialist services are encouraged to determine how this consultation may by facilitated, such as by phone, email or proforma remote consultations. An example of a proforma remote consultation for the initiation of HCV therapy has been developed by the Gastroenterological Society of Australia (GESA). This proforma and other educational materials and guidelines on HCV can be accessed on the GESA website
(www.gesa.org.au/index.cfm//resources/hepatitis-c-treatment).
The evaluation and management of patients with chronic hepatitis C are summarised in Flowcharts 1 and 2.
Patients with chronic hepatitis C who are more suitable for treatment under the direct supervision of a specialist liver service include those with cirrhosis, liver failure, HBV or HIV co-infection, multiple comorbidities, potential drug interactions or renal impairment.
Whichever management pathway is followed, it should be a collaborative decision between the patient, the family GP and the specialist.
Noninvasive assessment of liver fibrosis in chronic hepatitis C
Assessment of liver fibrosis status is essential to inform treatment options and long-term management of patients with advanced fibrosis and cirrhosis.
In the primary care setting, APRI (the AST to platelet ratio index) is a simple tool validated for predicting hepatic fibrosis and cirrhosis in patients with chronic hepatitis C. It is calculated using the formula:
APRI = (AST [IU/L] ÷ AST upper limit of normal [IU/L] × 100) ÷ platelet count [× 109/L]
An online calculator can be accessed at www.hepatitisc.uw.edu/page/clinical-calculators/apri. An APRI <1.0 has high specificity for exclusion of cirrhosis in patients with chronic hepatitis C.14
Transient elastography (FibroScan) is also well validated in patients with chronic hepatitis C and is an alternative or complementary test for assessing hepatic fibrosis by noninvasive means.11
Follow up of patients treated for chronic hepatitis C
The GP has an essential role in the follow up of patients treated for chronic HCV infection. All patients should have an HCV RNA test at least 12 weeks after the end of treatment to confirm eradication of HCV. The presence of detectable HCV RNA after treatment indicates treatment failure, which is usually due to the development of antiviral drug resistance. This situation is expected in approximately 5% of people being treated. Patients with treatment failure should be referred to a specialist for consideration of salvage therapy. There is no immunity to HCV, and even after successful eradication of HCV, patients at high risk of re-infection (e.g. HIV-positive patients) should be monitored with HCV RNA testing every 12 months and ALT measurement every three to six months so that reinfection can be diagnosed and treated.11
Patients with no detectable HCV RNA 12 weeks after treatment are considered cured of HCV infection. However, if the liver enzymes do not normalise, the patient may have another cause of liver disease (such as NAFLD) and should be further evaluated.
All patients determined to have cirrhosis on pretreatment assessment must have long-term surveillance for HCC (six-monthly liver ultrasound examinations and alpha-fetoprotein measurement).
Conclusion
Hepatitis B and C, along with nonalcoholic fatty liver disease and alcoholic liver disease, are challenges in primary practice and specialist settings. As the burden of liver disease in Australia increases, people at risk need to be identified to prevent the morbidity and mortality associated with chronic liver disease. Collaboration between community GPs and specialist services is essential in the long-term management of these patients. MT
COMPETING INTERESTS: Dr Pattullo has received honoraria for steering committee participation from MSD. Associate Professor Strasser has received honoraria for advisory board participation and speakers fees from Gilead Sciences, AbbVie, MSD, Bristol-Myers Squibb, Bayer, Norgine and Astellas.
References
- Deloitte Access Economics for The Gastroenterological Society of Australia/Australian Liver Association. The economic cost and health burden of liver diseases in Australia. Sydney: Deloitte Access Economics; 2012.
- Pattullo V, Strasser SI. Managing the rising burden of chronic liver disease: nonalcoholic fatty liver disease and alcoholic liver disease. Med Today 2017;
18(1): 2835. - Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology 2005; 42: 1208-1236.
- Gastroenterological Society of Australia – Digestive Health Foundation. Australian and New Zealand chronic hepatitis B (CHB) recommendations. 2nd ed. Melbourne: Digestive Health Foundation, Gastroenterological Society of Australia; 2009.
- Weinbaum CM, Williams I, Mast EE, et al. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm Rep 2008; 57: 1-20.
- Davison SA, Strasser SI. Ordering and interpreting hepatitis B serology. BMJ 2014; 348: g2522.
- Terrault NA, Bzowej NH, Chang K-M, Hwang JP, Jonas MM, Murad MH; American Association for the Study of Liver Diseases (AASLD). AASLD guidelines for treatment of chronic hepatitis B. Hepatology 2016; 63: 261-283.
- Visvanathan K, Dusheiko G, Giles M, et al. Managing HBV in pregnancy. Prevention, prophylaxis, treatment and follow-up: position paper produced by Australian, UK and New Zealand key opinion leaders. Gut 2016; 65: 340-350.
- Reddy KR, Beavers KL, Hammond SP, Lim JK, Falck-Ytter YT. American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology 2015; 148: 215-219.
- Perrillo RP, Gish R, Falck-Ytter YT. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology 2015; 148: 221-244; e223.
- Hepatitis C Virus Infection Consensus Statement Working Group. Australian recommendations for the management of hepatitis C virus infection: a consensus statement 2017. Melbourne: Gastroenterological Society of Australia; 2017.
- Baker D. Curing hepatitis C in general practice: a 12-step guide. Medicine Today 2016; 17(10): 14-22.
- Sievert W, Razavi H, Estes C, et al. Enhanced antiviral treatment efficacy and uptake in preventing the rising burden of hepatitis C-related liver disease and costs in Australia. J Gastroenterol Hepatol 2014; 29 Suppl 1: 1-9.
- Lin ZH, Xin YN, Dong QJ, et al. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: an updated meta-analysis. Hepatology 2011; 53: 726-736.