Pain after total knee replacement

Knee injuries and disorders
Pain
A 70-year-old man has ongoing, severe knee pain and difficulty mobilising after a total knee replacement for osteoarthritis. How should he be assessed and managed?
David is a 70-year-old retired accountant who presents to your general practice with severe right knee pain and difficulty mobilising seven days after having a right total knee replacement for osteoarthritis. He has been a patient at your practice for the past four years and his past medical history comprises depression, type 2 diabetes and hypertension, each of which is well controlled with a single first-line agent. He is overweight. Before having this operation he was requiring escalating doses of paracetamol and NSAIDS.
How would you assess David?
Answer: In Australia, where osteoarthritis is the most common musculoskeletal disorder and is the third largest contributor to disability,1 scenarios similar to David’s are increasingly being encountered by GPs. Total knee replacement (TKR) is one of the most cost-effective interventions for knee osteoarthritis to improve the quality of life of patients in Australia.1,2 As a result, the TKR rate has increased from 133/100,000 population in 2005/06 to 172/100,000 population in 2014/15.3 This is a pattern that is being replicated in the UK, the USA and most wealthy healthcare systems around the world.4,5
Enhanced recovery after surgery, or fast-track, programs are increasingly being adopted by healthcare services due to emerging evidence of improved recovery and reduced cost.6 Consequently, more TKR patients are being discharged from hospital earlier, and many of these patients require more complex acute pain management.7
In a survey of Australian patients who had had a TKR, most reported that the first two weeks after discharge from hospital was the most painful period of their postoperative course, and most consulted their GP during this time because of pain.8 Most of this cohort also reported their average pain as moderate to severe and were managing their pain with opioids despite significant side effects and without adequate nonpharmacological methods to manage pain.8
The causes of pain following TKR can be subclassified into intrinsic and extrinsic causes.9,10 Pain associated with stiffness or instability is most likely due to intrinsic causes including infection, instability, malalignment, soft-tissue impingement, arthrofibrosis, osteolysis, prosthetic loosening or failure and patellofemoral problems.9,10 Extrinsic causes include periprosthetic fracture, tendinopathy, bursitis, heterotopic ossification, vascular compromise, central or peripheral neuropathy, other musculoskeletal abnormality (hip, spine or ankle), psychosocial issues and inadequate analgesia.9,10
A thorough history for a patient such as David includes the indication for the operation, details of the operation and any early surgical complications, acute pain service strategies employed (regional anaesthesia techniques and analgesic regimens), a pain history regarding the current symptoms, a functional assessment including the patient’s compliance with prescribed home exercises, constitutional symptoms, localising infective symptoms, past medical history, medication history (current and preoperative medications), and psychological and social history.9,10
Your physical examination of David includes gait, palpation of the knee, active and passive range of motion of the knee including patella mobility and tracking, examination of adjacent musculoskeletal structures including the hip, lumbar spine and ankle, a neurological and vascular examination of the limb and a general examination for signs of infection.9,10
David’s early postoperative weight-bearing plain x-rays (AP, lateral skyline and long-leg alignment views) must be evaluated for alignment, component size and positioning, stress fracture, loosening, osteolysis, heterotopic ossification and unequal joint space.9 Additional investigations should be considered if indicated. A serum C-reactive protein level with or without synovial fluid microscopy, culture and sensitivity is important if infection is suspected. CT scans are more sensitive for rotational malalignment and periprosthetic fractures, and bone scans are more sensitive for component loosening or infection.9,10 At this time, consider referring the patient to their orthopaedic surgeon and any other specialist as appropriate.
How will you respond to David’s request?
Answer: Given the potential risk of opioid medication to both patients and the community, ‘universal precautions’ for opioid prescription, which have been adapted in the local Faculty of Pain Medicine guidelines (www.fpm.anzca.edu.au/documents), should always be applied.11,12 Before an opioid therapy trial is considered, a comprehensive biopsychosocial assessment and opioid misuse assessment must be performed, with subsequent optimisation of a multimodal plan toward active self-management.11,12
The assessment referred to above is consistent with a biopsychosocial assessment, but a more detailed description written by local experts is available.13 The Opioid Risk Tool is a quick, easy and well-validated tool that is most useful in an acute care setting as it provides excellent discrimination between patients with low and high risk of opioid misuse.7,14,15
A multimodal plan toward active self-management includes nonmedication therapies, multimodal analgesics (both nonopioid and opioid analgesics) and interventional therapies (if indicated).12 Evidence-based nonmedication strategies include education, pacing activity (including using the painful body part), graded exercise, sleep hygiene and psychological therapies, many of which may require the input of allied health providers.12Optimisation of such a comprehensive approach requires time and the co-ordination of a multidisciplinary team.
If an opioid therapy trial is considered appropriate, it is recommended that this involve a mutual agreement between the prescriber and the patient regarding clear goals (both symptomatic and functional) of the trial within an agreed time frame, regular assessment of the five As (analgesia [pain], activity [function], adverse effects, affect and aberrant behaviours) and a clear plan to appropriately wean opioid therapy should the goals not be achieved.11,12
At his current dose of oxycodone, David is experiencing inadequate desired effects with significant side effects. This would suggest that oxycodone is not the best opioid for him. It is important for all opioid prescribers to appreciate that there is a significant variability in individual patient responsiveness to each of the actions (analgesia, side effects and toxicities) of each opioid.16 This primarily relates to individual genetic factors and opioid receptor polymorphism.17 Also, it is important to appreciate that, on a population basis, there is little evidence to suggest any major differences in efficacy or adverse effects between any of the pure agonist opioids.7,18 Thus, optimal opioid therapy for each patient is only achieved after evaluating different pure agonist opioids until one is identified that provides the ideal balance of desired effects with minimal or no side effects.
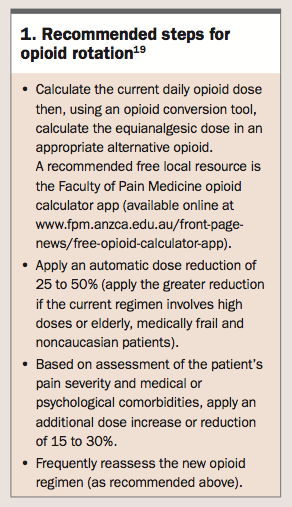
Opioid rotation, a change in opioid drug with the goal of improving outcomes, is indicated for David but caution is required.19 There is strong evidence that opioid rotation practices (which generally accounted for incomplete cross tolerance by reducing an equianalgesic dose by 25%) may be an important contributor to the increasing incidence of opioid-related fatalities.17 Revised consensus guidelines attempt to account for both interindividual variability in responsiveness and incomplete cross tolerance.19 The recommended steps for opioid rotation (which apply for all strong opioids with the exception of methadone or transbuccal fentanyl) are shown in Box 1.
{kind=link}
Extra caution should be applied when considering prescribing codeine and tramadol preparations, as pharmacogenetic variations in CYP2D6 are associated with significant risk of adverse effects, including death.7
As well as rotating to a different opioid agent, David may benefit from an ongoing prescription that comprises just an IR opioid preparation to be taken as needed. There is moderate evidence that pain-contingent dosing with oral IR opioids, when compared to time-contingent dosing with a combination of oral SR and oral IR opioids, results in significantly lower average daily opioid doses (97 mg versus 37 mg average daily dose oral morphine equivalent) and significantly lowers levels of opioid control concerns with no significant difference in analgesia.20 Also, transdermal opioid preparations are unsuitable for acute pain management due to their slow onset and offset as well as evidence of a high incidence of respiratory depression.18
Finally, consideration should be made to refer David to a local physiotherapist. There is strong evidence that, compared with the home exercise programs provided to patients in hospital (isometric strengthening exercises, exercises to regain active range of motion, gait training and stretches), additional outpatient exercise sessions based on functional activities with a subsequent home exercise program result in a significant small to moderate improvement in function for up to four months.21
David returns to your practice four months later requesting another prescription for IR oral morphine. Unfortunately he was lost to follow up and has not attended either of the appointments with the physiotherapist or orthopaedic surgeon. He confides that he has increased the daily dose of morphine to 120 mg, having been provided with prescriptions by a local emergency department and a number of after-hours GPs, each of which he consulted in a pain crisis. Despite the increased opioid dose, his right knee pain, walking and functional capacity remain the same as when you saw him last.
What options do you have for managing David’s opioid use?
Answer: Presenting to emergency departments, obtaining opioids from multiple prescribers and self-initiated dose escalation are all behaviours suggesting prescription opioid abuse.22 Other suggestive behaviours include frequent early appointments to a GP, recurrent lost prescriptions, frequently running out of medication early, refusal to pursue nonopioid treatments and focusing mainly on opioid issues during consultations.22 These are the aberrant behaviours that should be evaluated as part of the regular five As assessment that is recommended for use by all opioid prescribers.12
As a result of increased opioid prescribing, prescription opioid abuse with resultant fatalities is currently a global epidemic.23
In the USA from 1996 to 2011 medical use of prescription opioids increased by 1448% and prescription opioid abuse increased by 4680%. From 1999 to 2010 prescription opioid overdose deaths increased by 313%.23,24 In Australia the problem is not as large but the trend is similar: opioid dispensing increased 15-fold from 1992 to 2002, opioid-related hospitalisation increased 2.4-fold from 1998 to 2009 and death from accidental poisoning (from prescription opioids and illicit drugs) increased 1.7-fold from 2002 to 2011.25
Given the risk that David’s behaviour presents to both himself and the community, it is important to safely contain his prescription opioid use. An ongoing regular therapeutic relationship is fundamental to this aim, so empathy and maintenance of rapport are essential. This situation should prompt another detailed biopsychosocial assessment, as outlined above, to attempt to identify any precipitating and/or perpetuating factors contributing to this situation. This would include assessments by the orthopaedic surgeon and physiotherapist. Should such factors exist, addressing them may assist in managing David’s opioid use.
Regardless of whether such factors are identified, education and certain containment measures are advisable. First, David should be educated that there is no strong evidence for efficacy of long-term opioid therapy for chronic noncancer pain but there is good to fair quality evidence of harm, including opioid abuse and dependence, overdose, fractures, myocardial infarction and sexual dysfunction.26,27 Second, a revised opioid agreement should be reached with David that includes interval dispensing at short intervals as a condition and, ideally, physician-guided tapering as the goal. Finally, any future opioid prescriptions for David require an authority. Individual state and territory laws differ slightly, but in general in Australia an authority is required to prescribe Schedule 8 drugs if the duration exceeds two months or if the patient is suspected of being or known to be drug dependent.28
What is persistent postsurgical pain (PPSP) and what are the risk factors for its development?
Answer: Most patients who have a TKR for osteoarthritis experience a significant and sustained improvement in both knee pain and physical function, but there are a substantial number of patients who experience little or no benefit from the operation.29 You reassure David that, although he is currently in the latter group, there is potential to make functional gains while gradually reducing his opioid dose if he actively engages with the multidisciplinary team that you have brought together to manage his problem. If he struggles in achieving this goal, referral to a pain management clinic is recommended.
PPSP is defined as pain in the area of surgery that began after a surgical procedure and exists beyond the normal time for healing or the process of repair and is present at least three to six months after this initial event.30,31 There is strong evidence that the prevalence of PPSP after TKR is about 20% with an overall range in the studies of 10 to 39%.32-35 This figure is remarkably similar to the consistent 18% dissatisfaction rate after TKR identified in registry studies in Europe and North America.36
The mechanism of PPSP is complex and poorly understood but many models often involve central sensitisation.31 This is consistent with evidence that almost half of patients with PPSP after TKR have features of neuropathic pain.33
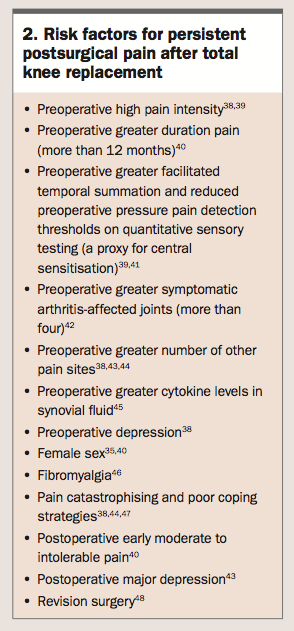
PPSP after TKR is associated with reduced function, increased rates of mood disorders and reduced quality of life.37 TKR is an elective procedure aimed at symptomatic and functional improvement, yet, clearly, it can make some patients worse. Unfortunately, there is limited evidence of any effective preventive treatments for PPSP after TKR, only conflicting evidence that perioperative gabapentinoids reduce neuropathic symptoms.35 To date, the focus of most research is on identifying risk factors for PPSP after TKR (Box 2).38-48
{kind=link}
It is theorised that preoperative screening and targeted strategies aimed at treating modifiable risk factors might reduce the incidence of PPSP after TKR. An alternative theory is that preoperative screening might improve selection of patients for whom surgical intervention might be reconsidered.PMT
References
1. March LM, Bagga H. Epidemiology of osteoarthritis in Australia. Med J Aust 2004; 180 (5 Suppl): S6-10.
2. Higashi H, Barendregt JJ. Cost-effectiveness of total hip and knee replacements for the Australian population with osteoarthritis: discrete-event simulation model. PloS One 2011; 6: e25403.
3. Australian Institute of Health and Welfare (AIHW). Admitted patient care 2013-14: Australian Hospital Statistics. Data tables. Chapter 6: What procedures were performed? Available online at: www.aihw.gov.au /publication- detail/?id=60129550483&tab=3 (accessed July 2017).
4. Bourlioufas N. Orthopaedic joint replacement surgery rates jump in developed nation as populations age: the bene ts speak for themselves. Australian Society of Orthopaedic Surgeons, 6 May 2016. Available online at: www.asos.org.au/orthopedic-surgery-rates-jump-in-developed-nation-as- populations-age.html (accessed July 2017).
5. Fingar K, Stocks C, Weiss AJ, Steiner CA. Most frequent operating room procedures performed in US hospitals, 2003-2012. Healthcare Cost and Utilization Project Statistical Brief No. 186. Rockville, MD: Agency for Healthcare Research and Quality, December 2014. Available online at: www. hcup-us. ahrq. gov/reports/statbriefs/sb186-Operating-Room-Procedures-United-States-2012. pdf (accessed July 2017)
6. Ibrahim MS, Khan MA, Nizam I, Haddad FS. Peri-operative interventions producing better functional outcomes and enhanced recovery following total hip and knee arthroplasty: an evidence-based review. BMC Med 2013; 11: 37.
7. Macintyre PE, Huxtable CA, Flint SL, Dobbin MD. Costs and consequences: a review of discharge opioid prescribing for ongoing management of acute pain. Anaesth Intensive Care 2014; 42: 558-574.
8. Chan EY, Blyth FM, Nairn L, Fransen M. Acute postoperative pain following hospital discharge after total knee arthroplasty. Osteoarthritis Cartilage 2013; 21: 1257-1263.
9. Mandalia V, Eyres K, Schranz P, Toms AD. Evaluation of patients with a painful total knee replacement. J Bone Joint Surg Br 2008; 90: 265-271.
10. Alves WM Jr, Migon EZ, Zabeu JL. Pain following total knee arthroplasty - a systematic approach. Rev Bras Ortop 2010; 45: 384-391.
11. Gourlay DL, Heit HA, Almahrezi A. Universal precautions in pain medicine: a rational approach to the treatment of chronic pain. Pain Med 2005; 6: 107-112. 12. Australian and New Zealand College of Anaesthetists (ANZCA), Faculty of Pain Medicine (FPM). Recommendations regarding the use of opioid analgesics in patients with chronic non-cancer pain. Melbourne: ANZCA and FPM, 2015. 13. Tsui SL, Chen PP, Ng KFJ (editors). Pain medicine: a multidisciplinary approach. Vol. 1. Hong Kong: Hong Kong University Press, 2010.
14. Webster LR, Webster RM. Predicting aberrant behaviors in opioid‐treated patients: preliminary validation of the opioid risk tool. Pain Med 2005; 6:
432-442.
15. Passik SD, Kirsh KL, C a s p e r D . A d d i ct io n - r el a te d a s s e s s m e n t t o o ls a nd p a i n management: instruments for screening, treatment planning, and monitoring compliance. Pain Med 2008; 9 Suppl 2: S145-S166.
16. Smith HS. Variations in opioid responsiveness. Pain physician 2008; 11: 237-248.
17. Webster LR, Fine PG. Review and critique of opioid rotation practices and associated risks of toxicity. Pain Med 2012; 13: 562-570.
18. Schug SA, Palmer GM, Scott DA, Halliwell R, Trinca J; APM:SE Working Group of the Australian and New Zealand College of Anaesthetists (ANZCA) and Faculty of Pain Medicine (FPM). Acute pain management: scienti c evidence. 4th edition. Melbourne: ANZCA, 2015.
19. Fine PG, Portenoy RK. Establishing ‘best practices’ for opioid rotation: conclusions of an expert panel. J Pain Symptom Manag 2009; 38: 418-425. 20. Von Korff M, Merrill JO, Rutter CM, Sullivan M, Campbell CI, Weisner C. Time-scheduled vs. pain-contingent opioid dosing in chronic opioid therapy. Pain 2011; 152: 1256-1262.
21. Minns Lowe CJ, Barker KL, Dewey M, Sackley CM. Effectiveness of physiotherapy exercise after knee arthroplasty for osteoarthritis: systematic review and meta-analysis of randomised controlled trials. BMJ 2007; 335: 812. 22. Ballantyne JC, Stannard C. New addiction criteria: diagnostic challenges persist in treating pain with opioids. Pain 2013; 21: 1-7.
23. Manchikanti L, Atluri S, Hansen H, et al. Opioids in chronic noncancer pain: have we reached a boiling point yet? Pain Physician 2014; 17: E1-E10.
24. Atluri S, Sudarshan G, Manchikanti L. Assessment of the trends in medical use and misuse of opioid analgesics from 2004 to 2011. Pain Physician 2014; 17: E119-E128.
25. Blanch B, Pearson SA, Haber PS. An overview of the patterns of prescription opioid use, costs and related harms in Australia. Br J Clin Pharmacol 2014; 78: 1159-1166.
26. Kissin I. Long-term opioid treatment of chronic nonmalignant pain: unproven ef cacy and neglected safety? J Pain Res. 2013; 6: 513-529.
27. Chou R, Turner JA, Devine EB, et al. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med 2015; 162: 276-286. 28. Royal Australasian College of Physicians (RACP). Prescription opioid policy: improving management of chronic non-malignant pain and prevention of problems associated with prescription opioid use. Sydney: RACP, 2008.
29. Wylde V, Dieppe P, Hewlett S, Learmonth ID. Total knee replacement: is it really an effective procedure for all? Knee 2007; 14: 417-423.
30. Merskey H, Bogduk N (editors). Classi cation of chronic pain. Second edition. International Association for the Study of Pain Task Force on Taxonomy. Seattle, WA: International Association for the Study of Pain Press, 1994.
31. Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth 2008; 101: 77-86.
32. Beswick AD, Wylde V, Gooberman-Hill R, Blom A, Dieppe P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open 2012; 2: e000435.
33. Pinto PR, McIntyre T, Ferrero R, Araújo-Soares V, Almeida A. Persistent pain after total knee or hip arthroplasty: differential study of prevalence, nature, and impact. J Pain Res 2013; 6: 691-703.
34. Drosos GI, Trianta lidou T, Ververidis A, Agelopoulou C, Vogiatzaki T, Kazakos K. Persistent post-surgical pain and neuropathic pain after total knee replacement. World J Orthop 2015; 6: 528.
35. Petersen KK, Arendt-Nielsen l. Chronic postoperative pain after joint replacement. Pain: Clinical Updates 2016; 24(3): 1-6.
36. Dunbar M, Richardson G, Robertsson O. I can’t get no satisfaction after my total knee replacement. Bone Joint J 2013; 95-B(11 Suppl A): 148-152.
37. Howells N, Murray J, Wylde V, Dieppe P, Blom A. Persistent pain after knee replacement: do factors associated with pain vary with degree of patient dissatisfaction? Osteoarthritis Cartilage 2016; 24: 2061-2068.
38. Lewis GN, Rice DA, McNair PJ, Kluger M. Predictors of persistent pain after total knee arthroplasty: a systematic review and meta-analysis. Br J Anaesth 2015; 114: 551-561.
39. Petersen KK, Arendt-Nielsen L, Simonsen O, Wilder-Smith O, Laursen MB. Presurgical assessment of temporal summation of pain predicts the development of chronic postoperative pain 12 months after total knee replacement. Pain 2015; 156: 55-61.
40. Puolakka PA, Rorarius MG, Roviola M, Puolakka TJ, Nordhausen K, Lindgren L. Persistent pain following knee arthroplasty. Eur J Anaesthesiol 2010; 27: 455-460.
41. Petersen KK, Graven-Nielsen T, Simonsen O, Laursen MB, Arendt-Nielsen L. Preoperative pain mechanisms assessed by cuff algometry are associated with chronic postoperative pain relief after total knee replacement. Pain 2016; 157: 1400-1406.
42. Perruccio AV, Power JD, Evans HM, et al. Multiple joint involvement in total knee replacement for osteoarthritis: effects on patient-reported outcomes. Arthritis Care Res 2012; 64: 838-846.
43. Wylde V, Hewlett S, Learmonth ID, Dieppe P. Persistent pain after joint replacement: prevalence, sensory qualities, and postoperative determinants. Pain 2011; 152: 566-572.
44. Dave AJ, Selzer F, Losina E, et al. The association of pre-operative body pain diagram scores with pain outcomes following total knee arthroplasty. Osteoarthritis Cartilage 2017; 25: 667-675.
45. Gandhi R1, Santone D, Takahashi M, Dessouki O, Mahomed NN. In ammatory predictors of ongoing pain 2 years following knee replacement surgery. Knee 2013; 20: 316-318.
46. D’Apuzzo MR, Cabanela ME, Trousdale RT, Sierra RJ. Primary total knee arthroplasty in patients with bromyalgia. Orthopedics 2012; 35: e175-e178. 47. Baert IA, Lluch E, Mulder T, Nijs J, Noten S, Meeus M. Does pre-surgical central modulation of pain in uence outcome after total knee replacement? A systematic review. Osteoarthritis Cartilage 2016; 24: 213-223.
48. Petersen KK, Simonsen O, Laursen MB, Nielsen TA, Rasmussen S, Arendt- Nielsen L. Chronic postoperative pain after primary and revision total knee arthroplasty. Clin J Pain 2015; 31: 1-6.