Persistent idiopathic facial pain: not just a diagnosis of exclusion

Facial injuries and disorders
Headache
The possible causes of orofacial pain are considerable and form a grey area between medicine and dentistry. An enigmatic condition formerly known as atypical facial pain has been renamed persistent idiopathic facial pain (PIFP) with defined diagnostic criteria. After the common causes of orofacial pain have been ruled out, then a diagnosis of PIFP can be considered.
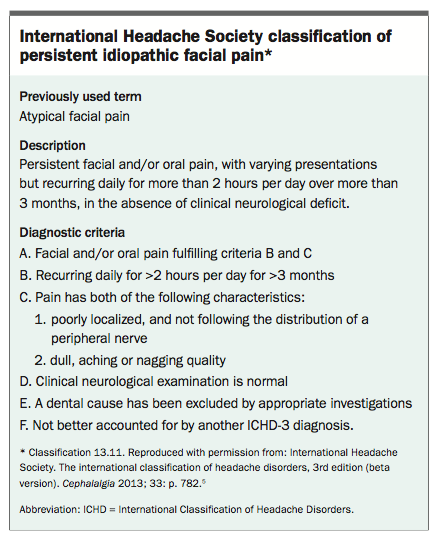
- Atypical facial pain is a ‘waste basket’ diagnosis that is no longer used. The new term is persistent idiopathic facial pain (PIFP).
- Defined diagnostic criteria for PIFP have been published but are not yet universally accepted.
- Patients with PIFP often visit multiple dental and medical practitioners in an attempt to diagnose and treat their pain, and undergo interventions or procedures without success or with exacerbation of the symptoms.
- PIFP should only be diagnosed after a thorough medical and dental history has been taken, then extra- and intraoral clinical examinations and appropriate imaging tests have ruled out other far more common causes of orofacial pain.
- Many patients with PIFP are middle to older aged women with comorbid psychological problems, yet no cause–effect relationship has been established.
- It is likely that PIFP is a neuropathic pain disorder involving abnormal peripheral nerve and central nervous system responses to a minor injury.
- Multidisciplinary assessment and pain management with pharmacological, nonpharmacological and interventional treatments are recommended.
- Future research is needed to establish clear diagnostic criteria and treatment strategies.
Picture credit: © BSIP/Oissonnet/Medical Images Model used for illustrative purposes only
Orofacial pain is common, with an estimated incidence in the general population of up to 26%.1 Orofacial pain can be severe and debilitating, resulting in serious effects on patients’ quality of life. Successful management of a patient seeking care for orofacial pain requires the clinician to first establish a diagnosis.2
Orofacial pain may be a symptom of disease of local structures, most commonly the teeth and sinuses, or of musculoskeletal, rheumatological, neurovascular, neuropathic and psychological causes. Pain can also be referred from distant structures, most commonly the neck, but even including the heart. Given this complexity, there are myriad causes of orofacial pain, and correct diagnosis begins with the GP at least being familiar with the most common conditions that may account for their findings on examination of the patient. Detailed history taking, intra- and extraoral physical examination and appropriate diagnostic tests are required for all patients presenting with orofacial pain. An interdisciplinary approach is often required to establish a correct diagnosis and thereby institute appropriate treatment.
Chronic orofacial pain symptoms that differ from those more commonly encountered have been described previously as atypical facial pain (AFP), often as a diagnosis of exclusion. The condition is now termed persistent idiopathic facial pain (PIFP). It is poorly defined and presents as both a diagnostic and therapeutic challenge for clinicians, as well as being a significant challenge for long-suffering patients with the condition. Until recently, a lack of understanding of the underlying pathophysiological mechanisms of PIFP has underpinned the difficulties in diagnosing and managing the condition.
It is not unusual for patients to consult multiple healthcare providers from different disciplines to find a solution for their orofacial pain problem. Patients presenting to a specialist orofacial pain clinic in Scandinavia had, on average, already consulted seven healthcare professionals including dentists, GPs, neurologists, ENT specialists, ophthalmologists, oral/maxillofacial surgeons and psychiatrists.3 Patients often become convinced that the pain is caused by an infection or cancer and that the clinicians thus far have been incapable of making a diagnosis. Hence, patients may seek out specialist after specialist in the hope of finding someone to diagnose and cure the pain. During this quest, a number of invasive dental and surgical treatments may have been attempted without benefit, and possibly with perpetuation or aggravation of symptoms.
The term AFP was first described in 1924 to differentiate it from trigeminal neuralgia.4 As the name implies, the diagnosis was typically made after excluding typical causes of orofacial pain such as local dental disease, cranial neuralgias and primary and secondary headache disorders. Indeed, absence of objective findings from the clinical examination, laboratory tests and medical imaging were considered to be the diagnostic criteria for AFP.
Owing to the vagueness of the term AFP and the proliferation of synonymous terms such as atypical facial neuralgia, atypical odontalgia, phantom tooth pain and migratory odontalgia, the International Association for the Study of Pain and the International Headache Society replaced the term AFP with PIFP. In 2013 the International Headache Society classification redefined PIFP (Box),5 but none of the published or proposed diagnostic criteria have yet been universally accepted or validated.
{kind=link}
PIFP is therefore best viewed as an idiopathic pain condition. The pain involves the trigeminal nerve distribution but does not fit criteria for other cranial neuralgias. The diagnosis is made by the report of continuous daily pain affecting the face and/or mouth for more than two hours per day without an obvious cause or mechanism. Patients are frequently misdiagnosed, or attribute their pain to a previous event, such as a dental procedure.
Epidemiology
At 0.03%, the estimated prevalence of PIFP in the general population is far lower than that of trigeminal neuralgia (0.3%).6 The incidence is unknown. PIFP mainly affects adults, and is rare in children. Clinical case studies indicate both sexes are affected, but most patients are middle to older aged women.7 Postulated risk factors include female sex, anxiety or depression, chronic widespread pain and a history of multiple surgical procedures.3
Clinical features
PIFP is usually poorly localised and of a deep, aching, pressing quality. It is typically, but not always, unilateral. The pain is of moderate to severe intensity, but this often fluctuates. At onset, the nasolabial and jaw areas are often affected. The pain does not follow dermatomal patterns and may spread elsewhere in the craniocervical regions. Patients often relate onset of pain to trauma or a dental procedure, such as root canal treatment or tooth extractions, but the pain may occur without any preceding injury.
The clinical examination and diagnostic work-up (e.g. laboratory findings and medical imaging studies) are usually unremarkable. Patients may report subjective feelings of altered sensation, but the pain is not associated with objective findings such as sensory loss, or other features of neuropathy such as allodynia and hyperalgesia. Cold weather, psychological stress, fatigue and dental treatment may aggravate the symptoms. PIFP may be comorbid with other pain conditions associated with central sensitisation, such as chronic widespread pain and irritable bowel syndrome. It is not unusual for patients with PIFP to also complain of headaches and neck and back pain. Psychological factors and psychiatric symptoms have been associated with PIFP and are common among patients with the condition, but the existence of a causal link between psychological factors and PIFP is contentious.8 Anxiety and depression scores are commonly high in PIFP patients, particularly those reporting high pain intensity.9 Therefore, psychological screening tests should be considered.10
Pathophysiology
Current opinion is that PIFP is unlikely to be a single clinical entity. It appears that both biological and psychological factors are involved. In some patients PIFP may be truly neuropathic, possibly related to a minor surgical procedure or a peripheral nerve injury in the orofacial region that cannot be locally demonstrated; in other patients the condition may be a focal manifestation of abnormal central nervous system processing and central sensitisation without an obvious aetiology.
PIFP and a related condition that is now termed painful post-traumatic trigeminal neuropathy (PPTTN) may form a continuum. It is possible that PIFP is induced by relatively insignificant trauma compared with PPTTN, which follows more obvious and significant trauma to the peripheral nerves. As compared to PIFP, positive or negative sensory changes associated with neuropathy, such as allodynia, hyperaesthesia or hypoaesthesia, are more prominent features of PPTN.
The term persistent dentoalveolar pain (PDAP; previously termed atypical odontalgia, phantom tooth pain, dental causalgia) has been applied to a continuous pain localised to one or more teeth, or a tooth socket after extraction, in the absence of any usual orodental cause. PDAP may be considered a more localised subform of PIFP, although the mean age at onset is younger and it occurs more equally among men and women. However, as there is a history of trauma in many cases, usually dental procedures, PDAP is more likely a subform of PPTTN. Potential risk factors for PDAP after endodontic treatment include extended duration of preoperative pain, female sex, presence of other chronic pain problems and a history of painful treatment in the orofacial region.11
Given that most patients with PIFP are either perimenopausal or menopausal women, and the known effect of oestrogen in other orofacial pain conditions, hormonal factors may be associated with the condition.12 The association between PIFP and certain psychiatric comorbidities, particularly depression, anxiety and high catastrophising, is well documented, but a direct aetiological link remains uncertain.13 The prevalence of psychiatric symptoms in patients with PIFP requires further study.
Underscoring the biological aspect, recent studies using quantitative sensory testing and brain imaging have been able to demonstrate specific central nervous system sensory abnormalities in patients with PIFP. It appears that hypofunction of dopaminergic pathways in the basal ganglia may contribute to PIFP and other related clinical pain conditions.14 About 20% of patients with PIFP show neurophysiological signs of trigeminal neuropathy compatible with subclinical neuropathic pain. Oral sensory abnormalities, in most cases thermal hypoaesthesia, have been shown in most patients, but 25% of patients with PIFP have normal findings in neurophysiological and thermal quantitative sensory testing studies.9,15,16 Current evidence supports the concept that, in most patients, PIFP is a subclinical trigeminal neuropathic pain that may arise from a minor, partial nerve trauma, pure peripheral small fibre neuropathy or a more central trigeminal system lesion.17
Differential diagnoses
PIFP is essentially a diagnosis of exclusion. Daily or near daily headaches are extremely common presentations in clinical practice. Primary headache disorders including chronic migraine, cluster headache and hemicrania continua may be confused with PIFP.
Careful medical and dental history taking, physical examination, laboratory studies and imaging studies are required to rule out more common causes of continuous orofacial pain. Both extraoral (cranial nerve, head and neck) and intraoral (teeth and oral soft tissue) examinations are needed to rule out local abnormalities and other sources of pain. As they are by far the most common causes of orofacial pain, orodental disease and myogenous temporomandibular disorders should be ruled out. Underlying primary or metastatic malignancy, diabetes, hypothyroidism, vitamin and folate deficiencies, oral infection, sinus infection and postherpetic neuralgia have been associated with continuous neuropathic-type pain and need to be ruled out. Demyelinating disease (either peripheral or central), connective tissue disease and other chronic pain disorders should also be considered.
Dental imaging including periapical and panoramic views is required to rule out dentoalveolar causes of pain. CT or MRI of the face, jaw and brain do not generally demonstrate any relevant abnormalities and are only indicated if the history and examination suggest a need (e.g. positive neurological signs).
Treatment considerations
The absence of any clear pathophysiological basis for PIFP precludes establishment of a treatment protocol.13,18 To date, there are no definitive curative therapies for PIFP; and, in addition, chronic pain is considered a disease entity where management rather than cure is the realistic outcome for patients.19
This may be difficult for patients to accept, particularly as they often believe there is undiagnosed malignancy or infection causing the problem. As mentioned earlier, these patients attend multiple healthcare practitioners of various backgrounds, frequently followed by invasive, unnecessary and costly procedures that fail. Patients with PIFP are probably best managed via a multidisciplinary chronic pain team.
Unfortunately, as very few randomised controlled clinical trials for the treatment of PIFP have been published, the provision of evidence-based treatment is problematic.20 However, studies have identified various pharmacological, nonpharmacological and interventional treatments that may provide moderate benefit.
In general, to date, the advocated treatments for PIFP are only partially successful and cannot be guaranteed. Patients should therefore be well educated about the nature of the condition and be prepared to live with residual pain. Psychological support is often necessary. Patients can be advised that in some people with the condition the pain ceases spontaneously. In others, treatment sees the pain gradually subside and eventually resolve; yet there are many patients in whom the condition persists and who require the continued use of medications and other strategies.
Pharmacological treatment
As is the case for other neuropathic pain syndromes, the use of tricyclic antidepressant medications (off label) may prove beneficial and is considered by many to be the first-line therapy for PIFP. Unless contraindicated, an upwardly tapering dose from 10 to 100 mg per day is prescribed.20,21
If tricyclics are contraindicated, poorly tolerated or ineffective, the use of a selective noradrenaline reuptake inhibitor (e.g. venlafaxine, duloxetine or mirtazapine; off label) is now advocated as second-line therapy.22 Alternatively, the alpha-2-delta ligands pregabalin or gabapentin can be trialled. Some authorities recommend that if a single agent is ineffective, then combinations can be used.
Nonpharmacological treatment
Considering the chronicity, resultant distress and the known association with psychological morbidity in patients with PIFP, psychological treatments have been recommended. Cognitive behavioural therapy as an adjunct to antidepressant medication has been shown to provide better outcomes than antidepressant medication alone.23,24 Due to a lack of controlled studies, there is limited evidence for psychological treatment for PIFP.25 Acupuncture, hypnosis and biofeedback have also been proposed and studied, but the evidence base to date is insufficient to warrant recommendation.26 More recently, the use of cannabinoids has been proposed but, again, further controlled studies are required.27
Interventional management
In recalcitrant cases, interventional procedures can be considered. Local anaesthetic block injections and pulsed radiofrequency (PRF) treatment of the sphenopalatine ganglion have both been shown to have moderate success in reducing PIFP symptoms. In one open trial of 30 patients with PIFP, 21% obtained complete relief and 65% rated their degree of pain relief between good and moderate. More than 50% of patients reported a 50% reduction in use of opioid medications.28 As a result of this and other studies, PRF can be considered as an interventional treatment for PIFP but higher level evidence is required.29,30
Neuromodulation with implanted peripheral nerve stimulators is also a promising option for patients with PIFP; but as with PRF, further randomised controlled trials with larger numbers of patients are needed.31 Botulinum toxin injections have also been studied as a treatment for patients with PIFP or other neuropathic pain conditions. Although the studies were small, the results were very promising and this treatment certainly warrants further study.32 Results of a small study in Taiwan suggest that low-energy (e.g. 800 nm wavelength) diode laser therapy may prove to be a useful alternative treatment for PIFP.33
Conclusion
PIFP, and the more localised PDAP, remain enigmatic chronically painful and debilitating conditions. Patients have often seen multiple health care providers and received unnecessary and ineffective or even harmful invasive procedures and costs.
PIFP should no longer be considered a ‘waste basket’ facial pain condition affecting patients with comorbid psychological problems. Recent neurophysiological evidence has confirmed that neuropathic pain mechanisms underlie PIFP. A diagnostic approach with a combination of thorough history taking, clinical examination and diagnostic testing is recommended.
It is important for GPs to be familiar with PIFP and to be able to differentiate it from the far more common causes of orofacial pain. Patients with the condition require interdisciplinary co-operation and conservative management. Referral to a multidisciplinary pain clinic, preferably one with an attending orofacial pain expert, is advised. Finding new, more effective treatments for PIFP will rely heavily on gaining further understanding of its underlying pathophysiology and on undertaking larger controlled trials of pharmacological and nonpharmacological treatments.PMT
References
55: 72-78.