Acute nontraumatic shoulder pain

Shoulder injuries and disorders
Pain
A 46-year-old abattoir worker develops shoulder pain while lifting carcasses at work. How should he be assessed and managed?
Red flag conditions that need to be excluded (and suggestive symptoms and signs) include:
- significant trauma (unexplained deformity, swelling or erythema)
- a major rotator cuff tear (significant weakness not due to pain, or bruising in the absence of trauma)
- concurrent or suspected malignancy
- inflammatory or infectious conditions (fever, night sweats, weight loss or arthralgia)
- referred pain from another condition (symptoms or signs suggestive of pulmonary or cardiovascular compromise, significant unexplained sensory or motor deficit).1,2
If any of these conditions are suspected then the patient should be referred promptly for specialist evaluation.2
posture
- active range of motion of the cervical spine
- active and passive range of motion of the shoulder joint
- isometric strength testing of the rotator cuff
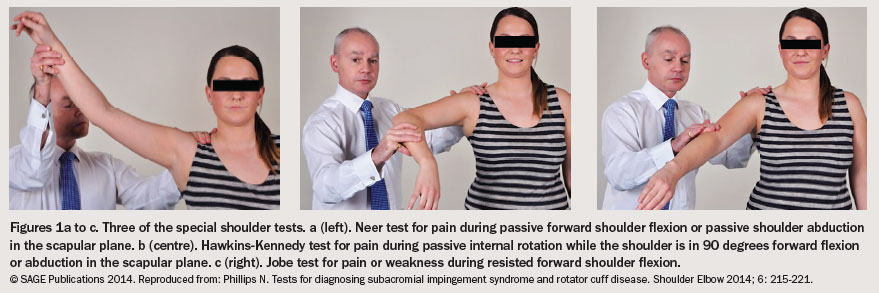
- special shoulder tests – the Neer impingement sign, Hawkins–Kennedy impingement sign, painful arc sign, Jobe test and infraspinatus muscle test (Box 1 and Figures 1a to c).3 Videos illustrating these tests are available online (e.g. at http://thepainsource.com).
{kind=link}
{kind=link}
It is important to be mindful that the examination may be limited by the patient’s pain. Minimising the patient’s discomfort can ensure rapport is maintained.
Individual special shoulder tests are not accurate for detecting rotator cuff disorder.4,5 However, combinations of these tests have a relatively high degree of accuracy.3,6 Positive findings for any combination of at least three of the above tests predicts rotator cuff disorder with a moderate degree of accuracy (sensitivity and specificity both approximating 75%).6 Positive findings for the combination of the Hawkins–Kennedy impingement sign, painful arc sign and infraspinatus muscle test have a high degree of accuracy for diagnosing rotator cuff disorder, with a post-test probability of 95%.3
{kind=link}
Across the western world, rotator cuff disorder is a common complaint among adult patients presenting to GPs. The incidence of rotator cuff disorder in this population in the Netherlands is 14.7 per 1000 patients per year.8 In the United Kingdom, the prevalence of rotator cuff disorder in the general practice patient population has been estimated at 16%.9 In both Australia and the UK, rotator cuff disorder is the third most common musculoskeletal condition of patients presenting to GPs.9,10
The prevalence of rotator cuff disorder is also influenced by occupational and environmental factors. Occupational factors that increase its prevalence include work that involves:11-13
- repetitive movements of the shoulder
- vibrational forces
- frequent positioning of the hands above shoulder level
- forceful movements
- high and low psychosocial job demands
- working in the fish and meat processing industry
- a low level of social support.
The prognosis of acute shoulder pain is worsened by a number of factors. There is strong evidence that a high pain intensity, a high shoulder pain and disability index (SPADI) score and a longer duration of a shoulder condition predict the persistence of shoulder pain.14 There is also moderate evidence that male sex, age greater than 55 years, perceived poor general health, increased sick leave utilisation, increased healthcare professional visits, the perception of high job demand and the perception of low social support also predict the persistence of shoulder pain.14 Workplace factors specific to predicting persistent shoulder pain include work involving greater forceful effort, awkward posture, high psychological demands and low decision latitude.15
All patients should be encouraged to maintain usual activity within the limits of pain, with reinforcing education on the strong evidence that early mobilisation of acute limb injuries is beneficial in terms of reduced symptoms, improved range of motion and return to work.20,21 Patients should also be reassured that conservative management of acute shoulder conditions leads to recovery in most patients (50% by six months, 60% by 12 months and 75% at 22 months).22,23
Analgesic medication is a recommended initial treatment in patients with significant pain associated with acute rotator cuff disorder.1,2,16 There is strong evidence that NSAIDs are superior to placebo in terms of effects on pain and function over the short term in patients with rotator cuff disorder.24-26 However, long-term prescription of systemic NSAIDs should be considered with caution as it is associated with infrequent but serious gastrointestinal and cardiovascular complications.27 Topical NSAID preparations may be a safer alternative as they have few systemic side effects and are effective relative to placebo in patients with acute musculoskeletal pain.28 Although there is strong evidence that paracetamol is an effective analgesic in patients with acute pain with fewer side effects than NSAIDs, there is no direct evidence in patients with acute rotator cuff disorder.1,25,29 Similarly, there is no evidence supporting use of opioid analgesics in patients with acute shoulder pain.26 If opioid analgesics are being considered in patients with chronic noncancer pain then it is advisable to consult the recommendations on their use from the Faculty of Pain Medicine, Australian and New Zealand College of Anaesthetists.30
Although there is no evidence that prescribed exercise has any adverse effect on acute rotator cuff disorder and it is recommended by many guidelines, there is mixed evidence of any clinical effect.1,16 Prescribed exercise generally comprises stretching, active range of motion and progressive resistance strengthening exercises. A good example of a comprehensive prescribed exercise regimen specific to rotator cuff disorder is available from the American Academy of Orthopaedic Surgeons (http://orthoinfo.org).31
A recent Cochrane review (published after the above guidelines) found strong evidence that the combination of manual therapy and prescribed exercise was no different to placebo and very weak evidence that prescribed exercise alone was no different to placebo, both in contradiction of the previous version of the review.32,33 Both reviews included studies of patients with acute or chronic rotator cuff disorder, making the results difficult to interpret for patients with the acute disorder. A previous systematic review that is more relevant to patients with acute rotator cuff disease found strong evidence that prescribed exercise may reduce pain in both the short and long term.25 It is important to note that in this population there is no significant difference in outcome between individualised or group exercise and home-based or physiotherapy centre-based exercise.1,34
Returning an injured worker to meaningful work as soon as possible is associated with a significant reduction in duration of occupational disability.1 In the acute phase of any workplace injury, the most effective interventions are offered at the workplace and include low-intensity, work-specific interventions such as ergonomic modifications, graduated activity upgrading and cognitive behavioural therapy.35 The input of specialist allied health professionals, occupational physicians and rehabilitation physicians is valuable in developing a return-to-work program. In patients with work-related acute upper limb disorders, there is moderate evidence that workplace accommodations (suitable duties, modified work, task redesign, ergonomic modifications) by an occupational therapist result in significantly improved productivity at three months and reduced sick leave at four to 12 months.36,37 Well-trained case managers can also have a significant positive impact for such patients, with moderate evidence of greater patient satisfaction, decreased symptom severity, increased function and an earlier return to work.38
On review at six weeks after the injury, John’s right shoulder pain is reduced to moderate mechanically evoked pain. He attributes the reduction to a short course of ibuprofen and ongoing paracetamol. He consulted a local physiotherapist and subsequently has performed daily shoulder strengthening exercises, but his active range of motion remains restricted by pain. John also responded to your encouragement to minimise any absence from work when you negotiated a two-week medical certificate. He returned to full-time work just one week after the injury but is only managing light duties having failed a brief trial of usual duties last week. He also continues to have difficulty with strenuous domestic activities and relies on the assistance of his brother-in-law. John is frustrated by his situation and wonders whether surgery or any other intervention might be helpful.
If a non-full thickness rotator cuff tear is identified then a maximum of two subacromial corticosteroid injections for short-term symptomatic relief can be considered, but the supportive evidence for this therapy is weak and it may suppress healing.1,2,16,39 Other minimally invasive or noninvasive interventions such as acupuncture, transcutaneous electrical nerve stimulation (TENS), therapeutic ultrasound and platelet-rich therapies are not recommended because of a paucity of supportive evidence.1,2,16,25,40-42
Referral to an orthopaedic surgeon is consistently recommended for patients with symptomatic, large (over 3 cm), full-thickness rotator cuff tears, with mixed recommendations for symptomatic patients with smaller full-thickness and non-full thickness tears. However, there is limited or no evidence supporting these recommendations.1,2,16 A Cochrane review of surgery for rotator cuff disorder found moderate evidence that there is no significant difference between open or arthroscopic surgery and conservative management.43 In contrast, there are a few low- to very low-quality surgical studies that have shown significant symptomatic improvement with rotator cuff repair, but only in patients with symptomatic, chronic, full-thickness rotator cuff tears without radiological evidence of muscle atrophy or fatty infiltration.16
Regardless of whether subacromial corticosteroid injections or surgical management are added to conservative management strategies, the persistence of shoulder pain or functional limitation for more than three months after onset of rotator cuff disorder should prompt consideration of referral to local specialist multidisciplinary pain medicine services. This especially applies to patients with significant pain, functional limitation or modifiable negative prognostic factors. PMT
COMPETING INTERESTS: None.
References
- Hopman K, Krahe L, Lukersmith S, McColl AR, Vine K. Clinical practice guidelines for the management of rotator cuff syndrome in the workplace. Sydney: University of New South Wales; 2013.
- Arroll B, Robb G, Kool B, et al. The diagnosis and management of soft tissue shoulder injuries and related disorders. Best practice evidence-based guideline. Wellington, NZ: New Zealand Guidelines Group, New Zealand Accident Compensation Corporation; 2004.
- Park HB, Yokota A, Gill HS, El Rassi G, McFarland EG. Diagnostic accuracy of clinical tests for the different degrees of subacromial impingement syndrome. J Bone Joint Surg Am 2005; 87: 1446-1455.
- Dinnes J, Loveman E, McIntyre L, Waugh N. The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review. Health Technol Assess 2003; 7: iii, 1-166.
- Hughes PC, Taylor NF, Green RA. Most clinical tests cannot accurately diagnose rotator cuff pathology: a systematic review. Aust J Physiother 2008; 54: 159-170.
- Michener LA, Walsworth MK, Doukas WC, Murphy KP. Reliability and diagnostic accuracy of 5 physical examination tests and combination of tests for subacromial impingement. Arch Phys Med Rehabil 2009; 90: 1898-1903.
- Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am 1995; 77: 10-15.
- van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis 1995; 54: 959-964.
- Urwin M, Symmons D, Allison T, et al. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis 1998; 57: 649-655.
- Britt H, Miller GC, Henderson J, et al. General practice activity in Australia 2014–15. General practice series no. 38. Sydney: Sydney University Press; 2015.
- Macfarlane GJ, Pallewatte N, Paudyal P, et al. Evaluation of work-related psychosocial factors and regional musculoskeletal pain: results from a EULAR Task Force. Ann Rheum Dis 2009; 68: 885-891.
- van Rijn RM, Huisstede BM, Koes BW, Burdorf A. Associations between work-related factors and specific disorders of the shoulder – a systematic review of the literature. Scand J Work Environ Health 2010; 36: 189-201.
- Keijsers E, Feleus A, Miedema HS, Koes BW, Bierma-Zeinstra SM. Psychosocial factors predicted nonrecovery in both specific and nonspecific diagnoses at arm, neck, and shoulder. J Clin Epidemiol 2010; 63: 1370-1379.
- Struyf F, Geraets J, Noten S, Meeus M, Nijs J. A multivariable prediction model for the chronification of non-traumatic shoulder pain: a systematic review. Pain Physician 2016; 19: 1-10.
- Herin F, Vézina M, Thaon I, Soulat JM, Paris C; ESTEV group. Predictors of chronic shoulder pain after 5years in a working population. Pain 2012; 153: 2253-2259.
- American Academy of Orthopaedic Surgeons (AAOS). Optimizing the management of rotator cuff problems: guideline and evidence report. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2010.
- Beaudreuil J, Dhénain M, Coudane H, Mlika-Cabanne N. Clinical practice guidelines for the surgical management of rotator cuff tears in adults. Orthop Traumatol Surg Res 2010; 96: 175-179.
- Henbest RJ, Stewart M. Patient-centredness in the consultation. 2: Does it really make a difference? Fam Pract 1990; 7: 28-33.
- O’Connor AM, Bennett CL, Stacey D, et al. Decision aids for people facing health treatment or screening decisions. The Cochrane Library; 2009.
- Nash CE, Mickan SM, Del Mar CB, Glasziou PP. Resting injured limbs delays recovery: a systematic review. J Fam Pract 2004; 53: 706-712.
- Mitchell C, Adebajo A, Hay E, Carr A. Shoulder pain: diagnosis and management in primary care. BMJ 2005; 331: 1124-1128.
- van der Windt DA, Koes BW, Boeke AJ, Devillé W, De Jong BA, Bouter LM. Shoulder disorders in general practice: prognostic indicators of outcome. Br J Gen Pract 1996; 46: 519-523.
- Bonde JP, Mikkelsen S, Andersen JH, et al; PRIM Health Study Group.
- Prognosis of shoulder tendonitis in repetitive work: a follow up study in a cohort of Danish industrial and service workers. Occup Environ Med 2003; 60: E8.
- van der Windt DA, van der Heijden GJ, Scholten RJ, Koes BW, Bouter LM. The efficacy of non-steroidal anti-inflammatory drugs (NSAIDS) for shoulder complaints. A systematic review. J Clin Epidemiol 1995; 48: 691-704.
- Australian Acute Musculoskeletal Pain Guidelines Group. Evidence based management of acute musculoskeletal pain. Brisbane: Australian Academic Press; 2003.
- Speed C. Shoulder pain. BMJ Clin Evid 2006; 2006: 1107.
- Moore RA, Derry S, McQuay HJ. Cyclo-oxygenase-2 selective inhibitors and nonsteroidal anti-inflammatory drugs: balancing gastrointestinal and cardiovascular risk. BMC Musculoskelet Disord 2007; 8: 73.
- Derry S, Moore RA, Gaskell H, McIntyre M, Wiffen PJ. Topical NSAIDs for acute musculoskeletal pain in adults. Cochrane Database Syst Rev 2015; (6): CD007402.
- Schug SA, Palmer GM, Scott DA, Halliwell R, Trinca J; APM:SE Working Group of the Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine. Acute pain management: scientific evidence. 4th ed. Melbourne: FPM ANZCA; 2015.
- Faculty of Pain Medicine (FPM), Australian and New Zealand College of Anaesthetists (ANZCA). Recommendations regarding the use of opioid analgesics in patients with chronic non-cancer pain. Melbourne: FPM ANZCA; 2015.
- American Academy of Orthopaedic Surgeons. Rotator cuff and shoulder conditioning program. 2012. Available online at: http://orthoinfo.org/topic.cfm?topic=A00672 (accessed April 2017).
- Green S, Buchbinder R, Hetrick SE. Physiotherapy interventions for shoulder pain. The Cochrane Library; 2003.
- Page MJ, Green S, McBain B, et al. Manual therapy and exercise for rotator cuff disease. The Cochrane Library; 2016.
- Kromer TO1, Tautenhahn UG, de Bie RA, Staal JB, Bastiaenen CH. Effects of physiotherapy in patients with shoulder impingement syndrome: a systematic review of the literature. J Rehabil Med 2009; 41: 870-880.
- Franche RL, Baril R, Shaw W, Nicholas M, Loisel P. Workplace-based return-to-work interventions: optimizing the role of stakeholders in implementation and research. J Occup Rehabil 2005; 15: 525-542.
- Martimo KP, Shiri R, Miranda H, Ketola R, Varonen H, Viikari-Juntura E.
- Effectiveness of an ergonomic intervention on the productivity of workers with upper-extremity disorders-a randomized controlled trial. Scand J Work Environ Health 2010; 36: 25-33.
- Shiri R, Martimo KP, Miranda H, et al. The effect of workplace intervention on pain and sickness absence caused by upper-extremity musculoskeletal disorders. Scand J Work Environ Health 2011; 37: 120-128.
- Feuerstein M, Huang GD, Ortiz JM, Shaw WS, Miller VI, Wood PM.
- Integrated case management for work-related upper-extremity disorders: impact of patient satisfaction on health and work status. J Occup Environ Med 2003; 45: 803-812.
- Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. The Cochrane Library; 2003.
- Green S, Buchbinder R, Hetrick SE. Acupuncture for shoulder pain. The Cochrane Library; 2005.
- Moraes VY, Lenza M, Tamaoki M, Faloppa F, Belloti J. Platelet‐rich therapies for musculoskeletal soft tissue injuries. The Cochrane Library; 2014.
- Page MJ, Green S, Mrocki MA, et al. Electrotherapy modalities for rotator cuff disease. The Cochrane Library; 2016.
- Coghlan JA, Buchbinder R, Green S, Johnston RV, Bell SN. Surgery for rotator cuff disease. The Cochrane Library; 2008.