Preventing and managing postherpetic neuralgia

Shingles
Pain
Postherpetic neuralgia (PHN) is the most common complication of herpes zoster. PHN is a neuropathic pain that is usually severe, with a significant impact on the daily functioning of patients, especially elderly patients whose independence can be threatened. PHN is difficult to treat, and in most patients a combination of systemic, local, interventional, behavioural and physical management will be required.
- Postherpetic neuralgia (PHN) is a late complication of herpes zoster.
- Clinically, pain persisting after the resolution of the herpes zoster rash should be regarded as PHN.
- Because of the complicated and varied pathogenesis of PHN, determining the best therapeutic approach is problematic.
- Risk factors for developing PHN include severe acute pain during herpes zoster, severe rash, ophthalmic involvement, increasing age and diabetes.
- Vaccination with live-attenuated varicella–zoster virus and actively managing the pain of herpes zoster reduce the risk of PHN.
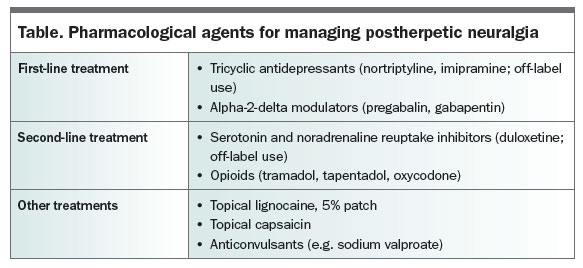
- A combination of first-, second-and possibly third-line medication options is often required to obtain the desired response in patients with neuropathic pain.
- Systemic treatments for PHN include tricyclic antidepressants, pregabalin and gabapentin as first-line options, and serotonin and noradrenaline reuptake inhibitors and opioids as second-line options.
- Lignocaine 5% skin patches are efficacious on areas where patients have allodynia.
Picture credit: © Phanie/Burger/Medical Images Model used for illustrative purposes only.
Postherpetic neuralgia (PHN) is the most common complication of herpes zoster, which is caused by the reactivation of the latent varicella–zoster virus (VZV; the cause of chickenpox) secondary to the waning of T-cell immunity. Reactivation occurs most commonly in elderly or immunocompromised patients. For clinical trials, PHN is defined as pain lasting more than three months (some will use six months) after the resolution of the herpes zoster rash. This is to allow for the possible natural resolution of the acute pain that occurs in a proportion of patients. Clinically, however, pain persisting after the resolution of the rash should be regarded as PHN.
PHN is an archetypal form of neuropathic pain, which is defined as pain resulting from a lesion or disease to the somatosensory nervous system. Patients who have PHN demonstrate hyperalgesia (increased pain from a painful stimulus), allodynia (pain from nonpainful stimuli), hyperpathia (more severe and prolonged pain than expected) and sensory loss. Patients may describe pain that is constant and paroxysmal, aching, deep, lancinating or burning, and may use words such as painful tingling or itching to describe dysaesthesias. Patients with a more severe response may demonstrate loss of motor function. The dermatome previously affected by the herpes zoster rash is associated with hypopigmentation, hyperpigmentation and scarring.
Pathogenesis
Herpes zoster causes an acute inflammatory response of the dorsal root ganglion and dorsal horn that is associated with acute ischaemia of these structures resulting in apoptosis and scarring. The virus migrates down the afferent nerve to produce inflammation of the terminal endings, resulting in the typical rash of herpes zoster. This peripheral inflammation can also cause scarring of the nociceptors and non-nociceptors in the skin. The resultant neuropathic pain will be due to a combination of deafferentation, conduction block, ectopic impulse generation (from the nociceptors, non-nociceptors, dorsal root ganglion and dorsal horn) together with peripheral and central sensitisation.1
In any patient and in any dermatome, the cause of ongoing neuropathic pain can be any combination of the above mechanisms, with any step predominating. As a result, determining what may be the best therapeutic approach in a patient is problematic. Attempts are being made to identify different sensory loss or gain profiles to determine the underlying mechanism of neuropathic pain and help improve the predictability of therapeutic responses.1
Risk factors for the development of PHN
Several investigators have studied risk factors for developing PHN.2 The most common risk factors for PHN are:
- severe acute pain during herpes zoster, including prodromal pain
- severe rash associated with herpes zoster
- ophthalmic involvement
- increasing age at the time of herpes zoster; the risk increasing from age 50 years
- diabetes (although the evidence is weak).
Depression and cancer have been shown not to be risk factors for PHN.
Prevention of PHN
The best method for preventing herpes zoster, and therefore PHN, is vaccination. A randomised controlled trial involving participants aged 60 years or older showed an overall reduction in the population incidence of herpes zoster of 51.3% and in the incidence of PHN of 66.5% with the current concentrated live-attenuated varicella vaccine.3 As reduced immunity to varicella–zoster virus starts to be noticeable from 50 years of age, vaccination from that time should be considered. Clinical guidelines recommend vaccination at least after 60 years.4 I recommend that patients be encouraged to be vaccinated from this age. On 1 November, 2016 the Australian Federal Government began funding a single dose of this vaccine for people between 70 and 79 years of age.
This live vaccine must not be given to an immunosuppressed patient, as this can lead to a generalised varicella infection. One death from this cause has been recorded in Australia.
Another vaccine under clinical trial promises to be more effective in further reducing the incidence of PHN. It is a herpes zoster subunit vaccine that combines a key surface glycoprotein of varicella–zoster virus, glycoprotein E, with a T cell-boosting adjuvant, AS01B.5
Actively managing the pain of herpes zoster reduces the risk of developing PHN. Antiviral medications should always be used in patients with herpes zoster, even after the recommended three-day window (off-label use). Antiviral use has been shown to reduce the severity and duration of herpes zoster. The antivirals valaciclovir and famciclovir are better absorbed and have better tissue penetration than aciclovir and may potentially reduce the incidence of PHN; however, evidence related to antiviral use and the incidence of PHN is conflicting.
Patients with herpes zoster should also be given a tricyclic antidepressant (off-label use) such as nortriptyline or imipramine, which have been shown to reduce pain and the risk of developing PHN. Avoid giving amitriptyline because of its side effect profile, especially in elderly patients. Further, appropriate standard analgesics should be used, beginning with paracetamol and NSAIDs. Corticosteroids may reduce the severity of pain in herpes zoster but have been shown not to reduce the incidence of PHN.
Management of PHN
As described above, the multiple aetiologies of this type of neuropathic pain make the management of PHN in any individual a clinical challenge. In addition, any centrally- acting medicine used in this more elderly and frail population is a limiting factor if dose escalation is required.
Pain management can be divided into systemic, local, interventional, behavioural and physical. In most patients, a combination of these will be required. Interventional therapies have a limited role and, being the realm of a pain medicine physician, are not described here.
Pharmacological management
Systemic medications for treating neuropathic pain are typically divided by the various published guidelines into first-line, second-
line and possibly third-line options (Table). However, in reality a combination of these is often required to obtain the desired response in patients.
{kind=link}
First-line treatments
Amitriptyline has been the most tested medicine in patients with neuropathic pain. However, because of the older age group of patients with PHN, nortriptyline and imipramine are the tricyclic antidepressants of choice for patients with PHN (off-label use). The starting dose for either drug should be 10 mg nightly, increasing gradually by 10 mg increments to a maximum dose of between 30 mg and 50 mg nightly.
The alpha-2-delta modulators pregabalin and gabapentin bind to calcium channels on the central terminals of the primary afferent nociceptors decreasing the release of neurotransmitters. The evidence for whether pregabalin or gabapentin is more efficacious in PHN is not conclusive, but both have been shown to be more than 2.5 times as likely to reduce pain by 50% or more compared with placebo.6 Some patients will respond to one and not the other, or develop side effects to one. Pregabalin tends to cause more sedation and cognitive dampening than gabapentin, but not always. Nocturnal sedation and analgesia may be beneficial because sleep deprivation caused by PHN can be significant and can lead to significant disability.
Pregabalin or gabapentin should be started at small doses and the dose increased gradually, generally on a weekly basis. The onset of an effect with pregabalin can be a week or longer in patients with chronic neuropathic pain, and gabapentin may take longer. Start pregabalin at 25 mg nightly or twice daily as a divided dose and increase by 25-mg steps to a maximum dose of 600 mg a day if needed and tolerated. Start gabapentin (which is on the RPBS but not the PBS for refractory neuropathic pain) at 100 mg nightly or three times a day as a divided dose, increasing by 100-mg steps to 900 mg a day. The onset of side effects should be monitored and the dose adjusted appropriately. The manufacturer-recommended doses of these drugs can be too aggressive and cause side effects; these can be averted with lower starting doses. Dosage adjustment should be slowed in patients with reduced renal function (especially eGFR <30 mL/min/1.73m2).
Second-line treatments
Serotonin and noradrenaline reuptake inhibitors (SNRIs) but not selective serotonin reuptake inhibitors (SSRIs) have shown some efficacy in patients with PHN. The onset of effect of an SNRI can be delayed. Duloxetine is the most studied and should be started at 30 mg (off-label use; duloxetine is indicated for diabetic peripheral neuropathic pain but not other neuropathic pain). Duloxetine is PBS subsidised, however, for use in patients with depression, which usually accompanies PHN.
Opioids should be used cautiously in patients with PHN. The choice of tramadol or tapentadol is based on their synergistic effect on the µ receptor and monoaminergic effects on neuropathic pain. Tramadol acts to inhibit serotonin reuptake but tapentadol does not. Both block noradrenaline reuptake. Tapentadol has a stronger opiate effect than tramadol and is classed as an S8 poison, but it still has 18 times less affinity to the µ receptor than morphine. Its combined µ opiate activity and noradrenaline reuptake inhibition provide better pain relief than other opiates in patients with neuropathic pain. Start tapentadol at 50 mg twice daily, titrating no more than weekly to a maximum dose of 250 mg twice daily of the slow release (SR) form.
Oxycodone has been recommended and widely used in patients with PHN as an adjunct, especially in the immediate-release and SR forms. However, a recent Cochrane review showed there was only very low-quality evidence that oxycodone (as oxycodone SR) is of value in the treatment of painful diabetic neuropathy or neuralgia, although many trials over short periods have shown benefit.7 There is only very poor evidence that a pure µ receptor opiate such as fentanyl has benefit in patients with neuropathic pain.8
Other treatments
Lignocaine 5% skin patches are efficacious on areas where patients have allodynia, but not on other painful areas because an intact but abnormal peripheral sensory system is required for them to work.9 A patch must be applied only to intact skin, after all the scabs from the herpes zoster rash are healed. Application for up to 12 hours a day is recommended if only one patch is being used. I advise patients to use a patch for longer, but tell them it must be removed for at least six hours so the skin will not macerate. Up to three patches can be used, although this is rarely needed and is expensive. Patches may be cut to the size of the affected area. Topical capsaicin in a high-concentration patch (not yet available in Australia) has been shown to provide good benefit in patients with PHN who respond; however, the quality of this evidence is weak.10
There is only weak evidence that sodium valproate is helpful in patients with PHN, and no evidence for other anticonvulsants.11 Sodium valproate should generally be started at 100 mg twice daily and increased weekly to the usual upper limit of 500 mg twice daily. The onset of effect can be delayed, making it a difficult drug to use.
Behavioural and physical pain management
PHN has a significant impact on the daily functioning of the patient, especially elderly patients whose independence can be threatened. The pain, sleep deprivation and grief for this loss of independence will have an impact on mood. Managing these psychosocial aspects with the assistance of psychological therapy, physiotherapy and occupational therapy is important to maximise the overall quality of care of these patients.
Conclusion
PHN is a severe and often debilitating pain following herpes zoster, and may lead to a reduced level of independence in the elderly. As pharmacological management is often difficult in older people the best management is prevention with vaccination, which reduces the incidence and severity of PHN. Monitoring the impact of the pain on the patient’s mood and function is as important as the pharmacological management. Close patient monitoring is needed to assess the response to therapy and the development of any adverse effects, which may necessitate dose or medication changes. Although the natural history of PHN is to improve despite often taking many months, the pain remains indefinitely in a proportion of patients.PMT
References
- Baron R, Maier C, Attal N, et al. Peripheral neuropathic pain: a mechanism-related organizing principle based on sensory profiles. Pain 2017; 158: 261-272.
- Forbes HJ, Thomas SL, Smeeth L, et al. A systematic review and meta-analysis of risk factors for postherpetic neuralgia. Pain 2016; 157: 30-54.
- Oxman MN, Levin MJ, Johnson GR, et al; Shingles Prevention Study Group. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med 2005; 352: 2271-2284.
- MacIntyre CR, Menzies R, Kpozehouen E, et al. Equity in disease prevention: vaccines for the older adults – national workshop, Australia 2014. Vaccine 2016; 34; 5463-5469.
- Cunningham AL, Lal H, Kovac M, et al; ZOE-70 Study Group. Efficacy of the herpes zoster subunit vaccine in adults 70 years of age or older.N Engl J Med 2016; 375: 1019-1032.
- Salah S, Thomas L, Ram S, Clark GT, Enciso R. Systematic review and meta-analysis of the efficacy of oral medications compared with placebo treatment in the management of postherpetic neuralgia. J Oral Facial Pain Headache 2016; 30: 255-266.
- Gaskell H, Derry S, Stannard C, Moore RA. Oxycodone for neuropathic pain in adults. Cochrane Database Syst Rev 2016; 7: CD010692.
- Derry S, Stannard C, Cole P, et al. Fentanyl for neuropathic pain in adults. Cochrane Database Syst Rev 2016; 10: CD011605.
- Mick G, Correa-Illanes G. Topical pain management with 5% lidocaine medicated plaster – a review. Curr Med Res Opin 2012; 28: 937-951.
- Derry S, Rice ASC, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database Syst Rev 2017; 1: CD007393.
- Wiffen PJ, Derry S, Moore RA, et al. Antiepileptic drugs for neuropathic pain and fibromyalgia – an overview of Cochrane reviews. Cochrane Database Syst Rev 2013; 11: CD010567.
COMPETING INTERESTS: Dr Gronow is on the Medical Advisory Board of Seqirus.